Download
1 / 70
870 likes | 2.81k Views
Hypoplastic Left Heart Syndrome (and the single ventricle repair). Henaro Sabino, MD Sibley Heart Center Cardiology at Children’s Healthcare of Atlanta; Emory University. CHEST PAIN, SYNCOPE. “I’M COMIN’ HOME!”. GOALS. Appreciation of history of Hypoplastic Left Heart Syndrome.

E N D
Hypoplastic Left Heart Syndrome (and the single ventricle repair) Henaro Sabino, MD Sibley Heart Center Cardiology at Children’s Healthcare of Atlanta; Emory University
CHEST PAIN, SYNCOPE • “I’M COMIN’ HOME!”
GOALS • Appreciation of history of Hypoplastic Left Heart Syndrome. • Basic anatomy & physiology. • (DE-mystify Hypoplastic Left Heart Syndrome.) • Understand the LOGIC behind the management of HLHS (& single ventricle lesions in general). • KEEP YOU ALL AWAKE FOR THE NEXT 1.25 HOURS.
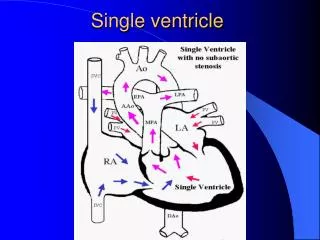
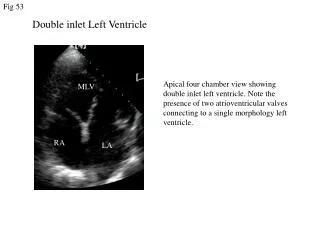
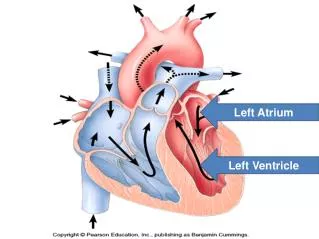
Hypoplastic Left Heart Syndrome • Spectrum of underdevelopment of the left ventricular cavity. • Have underdeveloped aortic & mitral valves (stenosis or atresia). • Left ventricle is unable to support systemic circulation (and, therefore, right ventricle is used as the single ventricle).
History of HLHS • First described by Maurice Lev in 1952. • Term used by Noonan & Nadas in 1958. • Options offered: • Comfort care • Staged palliative repair, i.e. “Norwood procedure” • First successful 3-stage completion in 1983 (after multiple surgeries from 1979). • Cardiac transplant • First successful cardiac transplant: Bailey, Nov. 1985
Xenotransplantation, “Baby Fae” • Dr. Leonard Bailey, Loma Linda University Medical Center, November 1984. • http://www.babyfae.com
HLHS Epidemiology • Low incidence of 1.6 to 3.6 per 10,000 live births, BUT causes 23% or cardiac deaths during 1st week of life and 15% during the 1st month of life. • Makes up about 2-4% of congenital heart disease. • More commonly males (55% to 67%). • With ONE affected child, recurrence risk is about 0.5% to 2%. • 12% prevalence of left-sided obstructive lesions in 1st degree relatives. • 15-30% incidence of genetic syndromes and extracardiac anomalies in patients w/HLHS. • Genetic markers: dHAND, HRT1, HRT2, NOTCH. • Moss & Adams, 2008.
PATHOPHYSIOLOGY • Cardiac development: “Flow begets growth.” • Altered flow through the left side of the heart: • Reduced/altered flow across the foramen ovale. • Aortic or mitral obstruction.
Typical Clinical Presentation • Known Congenital Heart Defect • Prenatal Diagnosis • Unknown Congenital Heart Defect • Normal pregnancy, labor and delivery • Clinically doing okay until the PDA closes ** • Cyanosis that does not improve with oxygen • Many have no other obvious anomalies
DUCTAL-DEPENDENT LESION • PDA needed to: • Provide systemic perfusion • HLHS ** • Critical aortic stenosis • Provide pulmonary blood flow • Tricuspid atresia • Pulmonary atresia • Provide mixing of oxygenated & deoxygenated blood • Transposition of the Great Vessels
Hyperoxitest • ABG is measured on room air. • Patient is placed on 100% oxygen (intubated) for 10-15 minutes, then ABG is repeated. • If problem is respiratory (i.e. hypoventilation), then PaO2 improves (usually above 200mmHg). • If problem is cardiac (i.e. right-to-left intracardiac shunt), there is little improvement of PaO2. • Primary pulmonary hypertension may also result in little improvement of PaO2. • (Oxygen may hasten closure of PDA!)
Positive Hyperoxitest • Seriously consider initiation of prostaglandin (PGE) at a low dose (0.03 mcg/kg/min) until diagnosis is confirmed.
Initial Assessment • ALWAYS • A - Airway • B - breathing • C – circulation CXR and ECG usually not very helpful in Dx.
Physical Findings • Comfortable or in distress? • Cyanosis w/out respiratory distress is cardiac until proven otherwise • Active or lethargic? • Cyanosis? • Degree - saturation usually <85% to be seen • Anemia makes cyanosis difficult to notice • Pallor • Vasoconstriction from circulatory shock • Perfusion and Peripheral pulses • End organs (i.e. watch UOP)
Respiratory Status • Tachypnea but with minimal distress…cardiac until proven otherwise.
Respiratory Status • Respiratory distress • Inability of the respiratory system to compensate for the metabolic acidosis • Concurrent respiratory disease • Unrelenting metabolic acidosis - decreased cardiac function • Exhaustion
AssistedVentilation • Intubate if: • Impending respiratory failure • Potentially not necessary to intubate just for PGE therapy if ground transport • Intubate for air transport in PGE dependent babies
Assisted Ventilation • Ventilation strategy • Volume ventilation if possible to maintain consistent minute ventilation in the face of changing lung compliance • Bigger tidal volumes compared to premature newborns (10 cc/kg); lower rates • No need to “over-ventilate” • “40/40/40 club”
Arterial Blood Gases • In congenital heart disease typically: • Compensated or partially compensated metabolic acidosis • Arterial PO2 usually low <50 with cyanotic heart disease…but not always • If PCO2 is rising, think respiratory failure - be ready to intubate!
Blood Gases Arterial Capillary Venous PH accurate accurate lower PO2 accurate invariable lower PCO2 accurate accurate higher HCO3(calculated) accurate accurate accurate
Oxygen • Oxygen is a drug - use it with respect • Oxygen is a pulmonary vasodilator • May worsen pulmonary congestion • Oxygen is a stimulus for the PDA to close • May worsen ductal dependent lesions by speeding up closure of the PDA • Oxygen is not bad
Saturation Monitoring • Oxygen saturation reflects tissue oxygenation and usually does not correlate with PO2. • With pulmonary hypertension will see differential cyanosis - shunts right to left across the PDA. • The number is not as important as the patient.
Prostaglandin Infusion • Purpose is to open the PDA if a ductal dependent lesion is suspected • Can be initiated before a definitive diagnosis is established • Need a secure IV (PIV, PIC, or UVC-central or in the liver) • Start at low dose 0.03 mcg/kg/min
Prostaglandins continued • Side effects - • Apnea - be prepared to intubate • Fever • Hypotension - have volume and inotropes available • Flushing
Access • Umbilical is preferred in a newborn • UVC – even if in suboptimal position • UAC • PIC line • PIV • AVOID groin line if possible
Fluid Resuscitation • Needed if poorly perfused • 5% albumin bolus (5-10 cc/kg) • Watch for and treat hypoglycemia - stress causes epinephrine release which increases utilization of glucose. • PRBC to treat anemia - optimize oxygen carrying capacity.
Hypotension • Check ionized calcium • Treat with 50-100mg/kg calcium gluconate or 10 mg/kg calcium chloride via central access • Dopamine 3mcg/kg/min increase as needed (no higher than 10 mcg/kg/min)
Metabolic Acidosis • Treat metabolic acidosis aggressively (base deficit < -3) • 1 meq/kg Na bicarbonate • Repeat blood gas
Renal function Urine output BUN/Cr Renal ultrasound Head ultrasound Liver function tests Coagulopathy Thrombocytopenia R/O sepsis Genetics Other Systems
Fetal Studies • Hornberger, 1995: 21 fetuses with prenatal echos that show left-sided obstruction (small mitral valve & ascending aorta) developed HLHS. • Critical aortic stenosis decreased blood flow through left heart LV dilation & dysfunction endocardial fibroelastosis (EFE) backwards flow across PFO LV stops growing & eventually shrinks
Case Presentation • Term infant born via SVD • Uncomplicated labor and delivery • APGARs of 8 at 1min., 9 at 5min. • Tachypnea noted at 12hrs of life.
Case Presentation • “Airway-Breathing-Circulation” • Respiratory rate (60-90 bpm) • Work of breathing (no retractions) • Saturations (80%) • Warm extremities; good cap refill
Case Presentation No obvious dysmorphic features. More Cardiac Exam Findings: • No murmur. • Single second heart sound (S2). • Hyperdynamic precordium.
Case Presentation • Urgent Cardiology Consult 404-256-2593!! • Cardiac History & Physical • Echocardiogram
Case Presentation • BUT: • No beds available at Egleston immediately • Need to manage infant for 24 hours before transport • NOW what do we do?
Case Presentation • Intravenous access • UVC (double lumen) • UAC • PIV • PIC Remember: AVOID groin lines
Case Presentation • Prostaglandins • 0.03 mcg/kg/min • Side effects • Apnea • Options ? • Intubate vs nasal cannula air
Case Presentation • Labs • Arterial (or venous) blood gas • Electrolytes (normalize) • CBC • LFT • Genetics • Lactic acid • Head and Renal ultrasound • ECHO/EKG
Case Presentation • R/O Sepsis • If no clinical suspicion or maternal indicators no need to start antibiotics • Follow ABG frequently (Q 4 hrs) • Monitor urine output • Monitor for acidosis • Watch for hypotension
Blood Pressure • Blood pressure - systolic and diastolic blood pressures are equally important…not just mean!! • Coronary flow to heart dependant on diastolic BP
Case Presentation • Saturations 95% • pO2 50 • Decreased urine output • Metabolic acidosis • Rising lactic acid What’s going on?!?