Download
1 / 24
250 likes | 320 Views
Hypoplastic left heart syndrome and the Rastelli procedure. Catherine Kim-Gavino, PGY4 Loyola University Medical Center. Admixture Lesions. Mixing of R & L circulations across a large VSD, ASD, PDA Admixed blood flows to pulmonary circulation Cyanotic with increased PBF.

E N D
Hypoplastic left heart syndrome and the Rastelli procedure Catherine Kim-Gavino, PGY4 Loyola University Medical Center
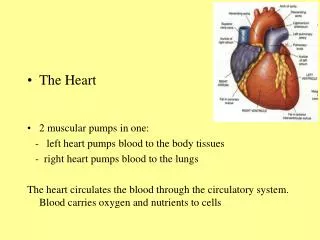
Admixture Lesions • Mixing of R & L circulations across a large VSD, ASD, PDA • Admixed blood flows to pulmonary circulation • Cyanotic with increased PBF
HLHS (Aortic Atresia) • Complex combination of cardiac malformations (8%) • Most common cause cardiac death 1st week of life • 4th most common cardiac malformation within 1st year of life • Behind VSD, d-TGA, TOF • M:F 2:1 • Invariably lethal if left untreated • 25% early cardiac deaths in neonate
Pathophysiology • Hypoplastic/absent LV, small sinuses of Valsalva, small Ao annulus/ascending Ao, LA, • 25% have a small MV or atresia • L-sided outflow tract obstruction • Variable severity • Systemic perfusion of aorta entirely thru PDA@ pulmonary pressures • Occasional ASD or VSD
HLHS • During systole: R-L flow through PDA to systemic circulation. • During diastole: L-R flow across PDA and retrograde flow through ascending Ao to perfuse coronaries. • PVR enters LA: restricted flow across atretic MV into hypoplastic LV. • LA blood shunted across interatrial communication (pinhole-sized FO to widely patent ASD). • Restricted FO flow + decreased flow through MV causes PVO obstruction. (typical presentation of neo w/severe CHF). • Nonrestrictive ASD allows larger-volume L-R shunt at atrial level and increased pulm artery BF. From www.childrenscentralcal.org
HLHS • Pulmonary, systemic, coronary circulation depends on RV • Rt-sided HF occurs rapidly, esp as ductus is closing (24-48 hrs) • Dusky infant in failure in first 48 hrs of life = HLHS • Maintain PDA patency with IV PGE1.
Imaging • Prenatal US: diastolic flow reversal in extremely narrow ascending Ao is diagnostic for HLHS. • Real-time echo: • sm, thick walled LV, sm MV w/restricted motion • Dilated RH/PA, lg PDA • Sm ascending Ao • CXR: • Moderate-marked CM • Globular cardiac silhouette suggesting combined chamber enlargement • PV congestion with interstitial/pleural fluid
Prognosis • CHF and death --> MI secondary to restrictive coronary flow or poor AV mixing. • Universally fatal with 80% patient dying within the first week. • Heart transplantation or staged Norwood procedure are alternative forms of therapy.
Norwood (3 stages) • Stage 1. At birth • Conduit RV to Ao root (Rastelli repair) • Divide PA from RV and ductus • Perfuse PA via Blalock-Taussig shunt • Stage 2. At 6 mos • Construct Glenn shunt (SVC to PA) to reduce volume load on RV • Stage 3. At 18 mos • Extracardiac Fontan. Direct blood from IVC & SVC thru RA to PA
But wait…. • Not all patients undergo this 3-stage palliative procedure. • If LV still functional, both ventricles can participate in cardiac circulation
Our patient, A.R. • 5 yo girl with past h/o resp distress soon after birth • CXR • Further w/u • Large VSD • Subaortic stenosis • Small ascending Ao • Coarctation of aorta
Rastelli surgery • Intracardiac conduit/baffle: • establishes continuity b/w LV and Ao • performed usu in DORV, forms of transposition (particularly w/VSD and subpulmonic stenosis). • Extracardiac conduit: • b/w RV and PAs during repair of TOF w/pulmonary atresia, TA, DORV. • Either a homograft AV w/segment of ascend Ao or a Dacron conduit with porcine AV is used.
A.R. • Treated with modified Norwood & Rastelli procedure: • Conduit from RV to pulmonary artery (w/AV) • Large baffle across VSD from LV to “neoaorta” • Constructed from Ao arch, descending Ao, MPA. • Ao root is anastomosed to neoaorta. • “Systemic valve” is PV • Closure of ASD • Repair of coarct.
LVOT SAG FIESTA RVOT
Complications • Obstruction b/w LV & Ao (VSD level) or other anastomotic sites • Incorrect placement of intracardiac baffle. • If VSD must be enlarged, may get complete HB, necessitating pacemaker. • Calcification of conduit/prosthetic valve ( conduit obstruction). • Obstruction/narrowing within conduit (neointimal fibrotic peel), thrombosis, periconduit abscess . • Pseudoaneurysms at anastomotic sites.
The End This is how I’m feeling, post-call
References • Kersting-Sommerhoffi BA, Seelos KC, Hardy C, Kondo C, Higgins SS, Higgins CB. The Evaluation of Surgical Procedures for Cyanotic Congenital Heart Disease by Using MR Imaging. AJR 1990; 155:259-266, • Bardo DME, Frankel DG, Applegate KE, Murphy DJ, Saneto RP. Hypoplastic Left Heart Syndrome. RadioGraphics 2001; 21:705-717 • Lonergan GL. Congenital Heart Disease. “Radiologic Pathology,” from the Armed Forces Institute of Pathology. Vol 3. 2006-2007. • Kuhn JP, Slovis TL, Haller JO. Caffey’s Pediatric Diagnostic Imaging. 10th ed. Mosby, Philadelphia. 2004