Download
1 / 1
20 likes | 127 Views
DELAYED DIAGNOSIS OF PERICARDIAL EFFUSION AND CARDIAC TAMPANADE Corey Chartan, MD, M. Caridad Davalos, MD, Satid Thammasitboon, MD, MHPE Baylor College of Medicine /Texas Children’s Hospital. Poster Title Researchers’/Presenters’ Names Institution/Organization/Company. Introduction. Case.

E N D
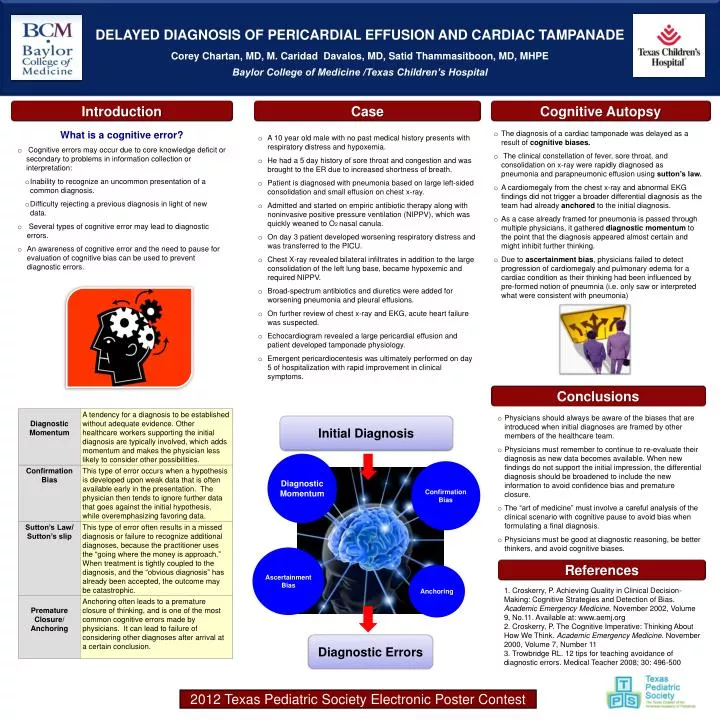
DELAYED DIAGNOSIS OF PERICARDIAL EFFUSION AND CARDIAC TAMPANADECorey Chartan, MD, M. Caridad Davalos, MD, Satid Thammasitboon, MD, MHPE Baylor College of Medicine /Texas Children’s Hospital Poster TitleResearchers’/Presenters’ NamesInstitution/Organization/Company Introduction Case Cognitive Autopsy Abstract (Click on the text to edit) • A 10 year old male with no past medical history presents with respiratory distress and hypoxemia. • He had a 5 day history of sore throat and congestion and was brought to the ER due to increased shortness of breath. • Patient is diagnosed with pneumonia based on large left-sided consolidation and small effusion on chest x-ray. • Admitted and started on empiric antibiotic therapy along with noninvasive positive pressure ventilation (NIPPV), which was quickly weaned to O2 nasal canula. • On day 3 patient developed worsening respiratory distress and was transferred to the PICU. • Chest X-ray revealed bilateral infiltrates in addition to the large consolidation of the left lung base, became hypoxemic and required NIPPV. • Broad-spectrum antibiotics and diuretics were added for worsening pneumonia and pleural effusions. • On further review of chest x-ray and EKG, acute heart failure was suspected. • Echocardiogram revealed a large pericardial effusion and patient developed tamponade physiology. • Emergent pericardiocentesis was ultimately performed on day 5 of hospitalization with rapid improvement in clinical symptoms. • What is a cognitive error? • Cognitive errors may occur due to core knowledge deficit or secondary to problems in information collection or interpretation: • Inability to recognize an uncommon presentation of a common diagnosis. • Difficulty rejecting a previous diagnosis in light of new data. • Several types of cognitive error may lead to diagnostic errors. • An awareness of cognitive error and the need to pause for evaluation of cognitive bias can be used to prevent diagnostic errors. • The diagnosis of a cardiac tamponade was delayed as a result of cognitive biases. • The clinical constellation of fever, sore throat, and consolidation on x-ray were rapidly diagnosed as pneumonia and parapneumonic effusion using sutton’s law. • A cardiomegaly from the chest x-ray and abnormal EKG findings did not trigger a broader differential diagnosis as the team had already anchored to the initial diagnosis. • As a case already framed for pneumonia is passed through multiple physicians, it gathered diagnostic momentum to the point that the diagnosis appeared almost certain and might inhibit further thinking. • Due to ascertainment bias, physicians failed to detect progression of cardiomegaly and pulmonary edema for a cardiac condition as their thinking had been influenced by pre-formed notion of pneumnia (i.e. only saw or interpreted what were consistent with pneumonia) Background Conclusions • Physicians should always be aware of the biases that are introduced when initial diagnoses are framed by other members of the healthcare team. • Physicians must remember to continue to re-evaluate their diagnosis as new data becomes available. When new findings do not support the initial impression, the differential diagnosis should be broadened to include the new information to avoid confidence bias and premature closure. • The “art of medicine” must involve a careful analysis of the clinical scenario with cognitive pause to avoid bias when formulating a final diagnosis. • Physicians must be good at diagnostic reasoning, be better thinkers, and avoid cognitive biases. Initial Diagnosis Diagnostic Momentum Confirmation Bias Ascertainment Bias References Anchoring 1. Croskerry, P. Achieving Quality in Clinical Decision-Making: Cognitive Strategies and Detection of Bias. Academic Emergency Medicine. November 2002, Volume 9, No.11. Available at: www.aemj.org 2. Croskerry, P. The Cognitive Imperative: Thinking About How We Think. Academic EmergencyMedicine. November 2000, Volume 7, Number 11 3. Trowbridge RL. 12 tips for teaching avoidance of diagnostic errors. Medical Teacher 2008; 30: 496-500 Diagnostic Errors 2012 Texas Pediatric Society Electronic Poster Contest