Download
1 / 22
400 likes | 1.06k Views
Sedation & Analgesia. PICU Resident Talk Stanford School of Medicine Pediatric Critical Care Medicine June 2010. Objectives. After this lesson, the participant will be able to: Differentiate between sedation and analgesia.

E N D
Sedation & Analgesia PICU Resident Talk Stanford School of Medicine Pediatric Critical Care Medicine June 2010
Objectives After this lesson, the participant will be able to: • Differentiate between sedation and analgesia. • Develop an appropriate sedation/analgesia plan, taking into consideration: airway, depth of sedation needed, time to onset of drug effect, duration of sedation/analgesia effect. • Describe the differences between distribution half life, elimination half-life and context sensitive half life.
Questions to ask yourself • Does patient need pain control or sedation? How can you tell which one? • Why does patient need sedation or pain control? Could the objective be achieved without it? Might agents for sedation or pain control make the patient worse (ie delirium)? • How quickly do you need effect? • How long do you need effect? • At what risk to the patient? • Are you prepared? Airway, BP support
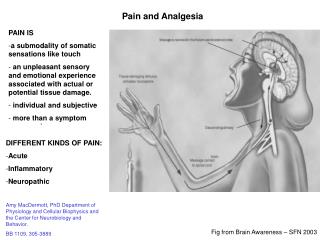
Definitions • Sedation--Reduction of anxiety, stress, irritability, or excitement by administration of a sedative agent or drug • Analgesia--the relief of pain
Levels of Sedation • Minimal Sedation (anxiolysis) • Normal response to verbal stimulus • Moderate Sedation (conscious sedation) • Depressed consciousness but response to verbal commands • Deep Sedation • Difficult to arouse • May need assistance w/ airway patency & ventilation • General Anesthesia • Not able to arouse even by painful stimulation • Impaired airway, ventilation & possibly cardiovascular function
Commonly used agents Analgesics Sedatives Chloral Hydrate Benzodiazepines (midazolam, lorazepam, diazapam) Propofol Barbituates (methohexital, thiopental, phenobarbital, pentabarbital) Etomidate • Acetaminophen • NSAIDS/ketorolac • Opioids (morphine, fentanyl, dilaudid) Analgesic and Sedative Effects Ketamine Dexmedetomidine Remifentanil
Opioids • Mediate pain by binding to the mu, kappa, and delta receptors. • Dose dependent sedative effect via kappa receptor • Dose dependent respiratory depression and decrease in blood pressure • Reversal agent: Naloxone
Comparitive Onset of Opioids 100 Hydromorphone 80 Morphine 60 site concentration Percent of peak effect Fentanyl 40 20 0 0 5 10 15 20 Minutes since bolus injection
Benzodiazepines • GABA agonist • Causes sedation/hypnosis, anxiolysis, amnesia • No analgesia • Dose dependent respiratory depression and decrease in blood pressure • Reversal agent: flumazenil
Chloral Hydrate • Sedative-hypnotic • Onset of action: 10-20 minutes • Peak action: 60 minutes • Duration 4-8 hours • No reversal agent • Unreliable in children over 3 years of age (Krauss Lancet 2006)
Propofol • GABA agonist—binds alpha subunit • Sedative only, no analgesic effects • Rapid onset and offset and no withdrawal • Onset: within 30 seconds • Duration: 3-10 minutes but depends on duration of infusion • PK follows 3 compartment model • Rapid distribution from blood into tissues • Rapid metabolic clearance from blood • Hepatic + extra-hepatic metabolism • Slow return to blood from peripheral compartment
Propofol • Propofol infusion syndrome—most often lactic acidosis, rhabdomyolysis, and circulatory collapse (Wysowski Anesthesia 2006, Cremer Critical Care 2009) • Propofol infusion syndrome typically occurs when high doses (greater than 67-83mcg/kg/min) are given for long periods of time (greater than 24 hours). (Roberts Critical Care Med 2009, Cremer Lancet 2001 and Cornfield Pediatrics 2002) • Not indicated for sedation in the PICU according to product label
Ketamine • “Dissociative” anesthetic • Works at multiple receptors—NMDA receptor antagonist, opiate receptor agonist • Bronchodilation effects (Hemmingsen Am J Emerg Med 1994) • Associated with hemodynamic stability and sometimes hypertension • Respiratory effort and airway reflexes maintained • Onset of action: 30 seconds to 1 minute • Duration of action: 5-30 minutes • Adverse effects: increased secretions, dysphoria, pychosis (may be improved with midazolam premedication)
Dexmedetomidine • Alpha-2 adrenergic agonist • Has both sedative and analgesic properties • Adverse effects: bradycardia, may excacerbate heart block, hypertension, hypotension
Etomidate • Sedative-hypnotic • Used primarily for procedures; doesn’t cause hemodynamic instability • Onset of action: 5-30 seconds • Peak action: 1 minute • Duration of action: 2-10 minutes • Adverse effect: Transient adrenal suppression (Wagner New England Journal 1984)
Barbiturates • Methohexital, thiopental, pentobarbital • GABA receptor agonist • Rarely used in PICU because of hemodynamic effects and because there is no reversal agent • Used for seizure burst suppression
Elimination Half Life versus Context Sensitive Half Life • Distribution half life (t1/2): the time required for plasma conc. to drop by 50% due to movement from central to peripheral compartment • Elimination half life (t1/2): the time necessary to metabolize/excrete 50% of the drug from the body after IV injection • Context Sensitive half life: Time for plama drug concentration to decrease by 50% after cessation of an infusion. Incorporates effects of redistribution into and out of peripheral compartments (3 compartment model).
Summary of Key Points • Be prepared to manage adverse effects when you give a sedative or analgesic drug • Have a plan! Know what is needed to achieve your goals. • Understand the pharmacokinetics
Cases • 1 year old intubated for ALI and pneumonia who needs sedation for arterial line placement. • 5 year old with elevated WBC count and mediastinal mass on Chest X-ray and oncology wants a chest CT. • 4 year old returns from OR after undergoing LTR. Needs to be sedated for a week.