Download
1 / 25
250 likes | 362 Views
Pakistan Polio Communication Review Recommendations Towards Complete Coverage. Pakistan Polio Communication Review Meeting Islamabad September 17-19, 2007. PEI In Pakistan: 2007 Overview. Tremendous gains have been made since the start of polio eradication activities in 1994 :

E N D
Pakistan Polio Communication Review RecommendationsTowards Complete Coverage Pakistan Polio Communication Review Meeting Islamabad September 17-19, 2007
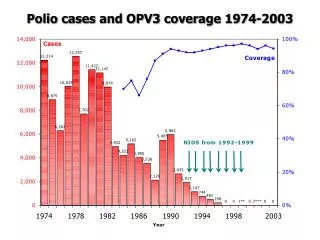
PEI In Pakistan: 2007 Overview • Tremendous gains have been made since the start of polio eradication activities in 1994 : • Average coverage rates at the provincial level are >95% across the country. • Sub-national variations exist. • Progressive decrease in cases since 1998.Total number of new cases in 2007 to date is 13. • Geographic and genetic localization of identified cases. • Overall sensitive surveillance system well over global certification standards. • Improving routine EPI coverage but sub-optimal coverage in certain areas.
Social Mobilization and Communication Activities: 2007 Overview • Strong coordination of partners leading to a successful national programme. • Comprehensive national strategy in place. • Communication activities an integral part of the programme. • mass media, advocacy, IPC, education and programme communication materials and other social mobilization activities.
Overall Programme Objective:Outstanding Challenges Some areas of sub-optimal coverage remain. • Reasons for missed children include: • Quality of Operations • Inaccessibility (area and households) • Mobile Populations • Refusals • Under-utilization of programme data linking SIA outcomes with communication activities
Recommendation Area: Maintaining Achievements • High Coverage Overall • Need to sustain acceptance in populations already accepting vaccine through message development targeted at emerging concerns (i.e. over vaccination, multiple campaigns) • Quantify number and location of missed children due to inaccessibility due to security using complete denominators • Good surveillance and regular reviews • Expand community-based AFP Surveillance • High level political commitment • Strengthen translation into action in particular in high risk districts and sub-districts of the remaining three endemic provinces to demonstrate ownership
Recommendation Area: Maintaining Achievements • Broad-based media campaign achieving high level awareness (TV, radio, print media including new approaches, e.g. polio true stories) • Assess impact of the current strategy elements to guide allocation of resources and activities (such as production/use of posters) • Strengthen provincial leadership for programme communication activities and planning.
Recommendation Area: Focus Strategies in High Risk Areas • Strengthen data driven communication strategies at sub-district level: • use Control Room and PCM data to identify shortfalls in SIA performance and analyze trends. • Include previous SM/C activities in trend analysis to assess impact and develop indicators by which to assess future impact. • Modify SM/C activities to according to impact • Conduct program activity • Link impact data from SM/C activities to trends • Emphasize focus of communication activities on sub-district levels in high risk areas (UCs/Areas)
Strategic Approach to Communication Activities High number of communication activities are being conducted. The next phase of the programme requires intensification and evidence based strategy which should include: • Retrospective desk review of SM/C activities related to programme achievements • Planning and monitoring for impact; developing indicators • Modifying SM/C activities
Strategic Approach to Communication Activities Previous Interventions: communication Strategy/Intervention: Jirga, press release, mosque announcements, community meeting, DCHO • Trend analysis to identify reasons and patterns of missed children: • Inaccessibility (to area/household) • Performance of teams (IPC, no team, not available) • Refusals (perceptions, mis-information, demand) • Impact of previous interventions Locally appropriate strategy identified(DSO, SO, CSP, DHCO & community) Implement and measure communication strategy (s) Implement program activity Surveillance data Collect Data SIA data (control room, PCM) over time
Example 1: “No Team”Inadequate access for teams to children under six months. • Analyze the data to identify the cause of the access problem at the sub-district level • Review current SM/C activities to look for evidence of impact (i.e. decrease in proportion of ‘no team’ in PCM, increase in general or under 6 months coverage) • Modify SM/C responses and measure new impact going forward e.g.: • SM/C involving peri-natal care providers (proportion of TBAs/community mid-wives briefed, increase in birth registration) • Engagement with mothers in the community to increase awareness of EPI and polio (rate of demand for EPI amongst mothers increased)
Example 2: RefusalStrategic Approach • Review prior programme data to identify trend • Distinguish persistent or transient refusal • Identify specific causes of refusal e.g. • negative media, misconception, fatigue, too much OPV, religious objection, demand related • Analyze relationship between SM/C activities and refusal trends (increase in convincing, decrease in refusal) • Modify SM/C activity accordingly and measure impact going forward • Link back to programme data
Implement and measure communication strategy (s) • Provincial level support to support training prior to campaign • Mobilize quality CSP, DSO, DCHO to area during campaign • Conduct jirga meeting (tribe A) in UC 5 inviting all religious leaders two days before SIA, • Conduct jirga (tribe B) in UC 3 with different leaders two days before SIA Strategic Approach to Communication Activities • Trend analysis to identify reasons and patterns of missed children: • Low recording of absent or unavailable children by vaccination teams • Refusals: most refusals are located in UC 5 and are primarily due to misconception of two local religious leaders • UC 3 had few refusals also due to mis information • Locally appropriate strategy identified • Training conducted in presence of high level support, focus on IPC and using tally sheets of previous rounds in training • UC 5 and 3 are of two different tribes organize jirga with objective of gaining access to community communication Strategy/Intervention: Jirga meeting held in UC 3, attended by 15 community leaders, one week before the campaign Surveillance data SIA data (control room, PCM) over time Conduct SIA Conduct SIA
Recommendation Area: Training • Better use SIA data to identify gaps in vaccinator team performance related to: • Access to household • Quality of recording (NA, Refusals) • Supervision and Monitoring • Social Mapping
Recommendation Area: Training • Building on existing modules and training programmes, focus on: • Using previous SIA data relevant to the area of the teams being trained • Analyzing and plotting local realities (e.g. areas of low coverage or refusals) using social maps • Strengthen IPC negotiating skills using past SIA household case studies • Build morale by providing programme overview and global updates • Monitor impact of improved trainings
Recommendation Area: Human ResourcesProvincial Level There is a gap in strategic communication capacity and leadership at the provincial level. • Create and fill immediately 3 long-term Provincial-level Programme Communication Specialist Posts • Skills should include: • Data analysis and communication strategy development with focus on high risk districts • Experience in communication, M&E and polio
Recommendation Area: Human ResourcesProvincial Level (Continued) • The post requires an independent critical analyst working as part of the provincial team (GoP, WHO, UNICEF). • The specialist should report regularly to the Federal level on progress and impact of communication strategies.
Recommendation Area: Human ResourcesDistrict Level • Ensure that ALL high-risk districts have DHCSOs. • Positions should be filled immediately • DHSCOs should be provided regular training on communication strategies and fully utilize the expertise of the provincial specialist.
Recommendation Area: Follow-up to Communication Activities • Hold regular team leader meetings attended by partners with report backs on communication by the provincial communication specialists. • Expand mandate of TAG to include substantial component of communication: • to include a communication expert on the TAG • Provincial Communication Specialists to report regularly to the TAG
Summary • Sustain achievements of the programme • Intensification phase of communication focused on sub-district strategic approach • Link data with SM/C activities • Develop and monitor indicators • Refine and modify approaches accordingly • Focus training on IPC quality, use of data in training and social mapping. • Increase capacity and leadership for provincial and district communication urgently. • Ensure adequate follow-up through regular meetings, reporting and TAG.