Download
1 / 16
160 likes | 262 Views
Intravenous Erythropoietin in Patients with ST-Segment Elevation MI. -- Study performed by: Najjar et al -- Presented by: Jay Hall PA-SII, Ali Rahimi MD . JAMA, May 11 2011 Vol 305, No. 18. Erythropoietin. 165-amino acid glycoprotein hormone

E N D
Intravenous Erythropoietin in Patients with ST-Segment Elevation MI -- Study performed by: Najjar et al -- Presented by: Jay Hall PA-SII, Ali Rahimi MD JAMA, May 11 2011 Vol 305, No. 18
Erythropoietin • 165-amino acid glycoprotein hormone • produced by peritubular capillary endothelial cells in the kidney and liver • secretion is regulated by oxygen levels • Main function regulates RBC production through the CFU-E (colony forming unit) which is a RBC precursor • Exhibits pleiotropic effects including angiogenisis and protects vs. apoptosis • Receptors on cardiocytes • Preclinical data showed cardio-protective roll, decreased infarct size, reduce apoptotic cells and reduce cardiocyte loss
Goal of Study • To evaluate the safety and efficacy of a single intravenous bolus of epoetinalfa in patients with a STEMI
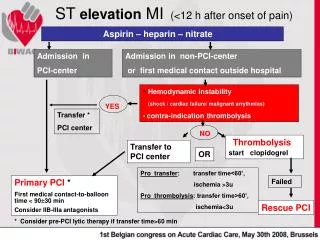
Design • Prospective, randomized, double-blind placebo controlled trial. • The REVEAL trial: 28 US sites between October 2006 – February 2010 included 222 patients with STEMI who underwent PCI as primary reperfusion strategy. • Patients were randomly assigned to treatment with intravenous epoetinalfa or matching saline placebo.
Design • Inclusion: STEMI with thrombolysis in mycoardial infarction, underwent successful PCI within 8 hours of ischemia. • Exclusion: h/o LV dysfunction (LVEF < 50%), MI, CABAG, revascularization of culprit aa. • Prevention of confounding infarct size • Epoetinalfa or saline placebo was administered within 4 hours after PCI • Restoration of flow to grade 2 or greater
Design • Patient underwent cardiac magnetic resonance imaging (CMR) to evaluate • LV volume – ESV, EDV • LV mass • LV function – LVEF • Contrast for infarct size
Endpoints • Primary Endpoints • Territory of the infarct size • Secondary Endpoints • LV remodeling (LV ESV, EDV, LVEF) • Safety Endpoints • Vitals, HgB, Recitculocytes, Clinical events
Results • Infarct size measured 2-6d and 12 +2 weeks following medication administration did not differ between epoetin and placebo • In either unadjusted or adjusted (age, artery) • Infarct mass did not differ at either time point • LVEF, LVESV, LVEDV indexed to BSA did not differ at any point • LV Mass indexed to BSA was statistically significant (P < 0.05)
Results • Subgroup analyses showed that age group may modify epoetin effects on infarct size. • In patients older than 70 the infarct size was LARGER on all CMR exams after receiving epoetinalfavs placebo • Results unchanged when adjusted for DM (which was the only significant difference between the groups)
Results • Participants receiving epoetinalfa had a higher incidence of adverse events • Epo: 69/125 {55.2%; 95% CI, 46.05-64.10%} • Plac: 40/97 {41.2%; 95% CI, 31.33%-51.69%} P=.04 • Also higher incident of serious adverse event • 20.0%; 95% CI, [13.38-28.09%] vs. Placebo 10.3%; 95% CI [5.06-18.14%] P=.05
Results • Of the 125 patients who received epoetinalfa, 5 experienced death, MI, stroke or stent thrombosis vs. 0 in 97 placebo patients • 4.0% [95% CI, 1.31-9.09%] P=.04
Conclusion • A single bolus of 60,000 U of epoetinalfa in patients with STEMI given within 4 hours of PCI does not reduce infarct size and is related with higher adverse cardiac events • Furthermore it was shown to increase infarct size in patients aged 70 and older.