Download

1 / 59
1.04k likes | 2.19k Views
INJURIES TO BIRTH CANAL. INJURIES TO BIRTH CANAL. NOT SO UNCOMMON – SPONTANEOUS or ASSISTED DELIVERIES DEPEND UPON THE CARE PROVIDED BY THE OBSTETRICIAN AVOIDANCE, EARLY DETECTION & PROMPT MANAGEMENT – KEY TO REDUCE SIGNIFICANT MORBIDITY. INJURIES TO BIRTH CANAL. CLASSIFIED:

E N D
INJURIES TO BIRTH CANAL • NOT SO UNCOMMON – SPONTANEOUS or ASSISTED DELIVERIES • DEPEND UPON THE CARE PROVIDED BY THE OBSTETRICIAN • AVOIDANCE, EARLY DETECTION & PROMPT MANAGEMENT – KEY TO REDUCE SIGNIFICANT MORBIDITY
INJURIES TO BIRTH CANAL • CLASSIFIED: • INJURIES TO BONY PARTS i) Injury to Symphysis Pubis ii) Injury to Sacro-coccygeal Joint iii)Injury to Sacro-iliac Joint • INJURIES TO SOFT TISSUE i) Injury to Vulva ii) Perineal Tears iii)Laceration of Vagina & Cervix iv)Rupture of Uterus
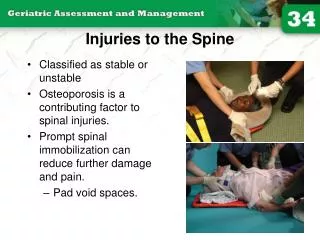
INJURIES TO BONY PARTS • INJURY TO SYMPHYSIS PUBIS: • DURING FORCIBLE EXTRACTION OF THE HEAD BY FORCEPS OR IN BREECH DELIVERY • NOT SO SERIOUS • URETHRA & BLADDER MAY BE INVOLVED – COMPLICATE THE CASE
INJURIES TO BONY PARTS • INJURY TO SYMPHYSIS PUBIS: • DIAGNOSIS:PAIN AT PUBIC REGION or MOVEMENT GAP MAY BE FELT TENDER PUBIC SYMPHYSIS • TREATMENT: BED REST FOR 2-3 WEEK ANALGESICS FIRM BINDER AROUND THE PELVIS BLADDER CARE
INJURIES TO BONY PARTS • # & DISLOCATION OF COCCYX: • DURING EXTRACTION WHERE SUB-PUBIC ANGLE IS NARROW • PAIN AT THE REGION OF COCCYX WHILE SITTING • MOBILE OR DISPLACED COCCYX • EXCISE THE COCYX
INJURIES TO BONY PARTS • INJURY TO SACRO-ILIAC JOINT: • Result after injury to Symphysis Pubis, Symphysiotomy or Pubiotomy • Ligaments are torn & Flaring out of the iliac bones • Do not support pelvis- can’t use limbs • Bed Rest; Straping of pelvis for 2-3 weeks
INJURIES TO SOFT TISSUE • INJUR TO VULVA: • MINOR TEAR OF LABIA MINORA, FOURCHETTE COMMON NO TREATMENT • VULVAL HEMATOMA: BLEEDING FROM PARAVAGINAL VEINS TENSE, BLUISH & TENDER LARGE:INCISION & CLOTS REMOVED
INJURIES TO SOFT TISSUE • PERINEAL TEARS: • GROSS INJURY IS DUE TO MISMANAGED 2ND STAGE OF LABOUR • ETIOLOGY: • OVER STRETCHING OF PERINIUM • RAPID STRETCHING OF PERINIUM • INELASTIC PERINIUM
INJURIES TO SOFT TISSUE • PERINEAL TEARS: DEGREES: • First-degree: involve the perineal skin, and vaginal mucosa • Second-degree: 1st degree and the fascia and muscles of the perineal body • Third-degree: 2nd degree and involve the anal sphincter. • A fourth-degree: extends through the rectal mucosa to expose the lumen of the rectum.
THIRD DEGREE PERINEAL TEAR FOURTH-DEGREE PERINEAL TEAR
INJURIES TO SOFT TISSUE • PERINEAL TEARS: • PREVENTION: • LIBERAL USE OF EPISIOTOMY • PROPER CONDUCT OF LABOUR DURING 2ND STAGE • PERINEAL SUPPORT DURING 2ND STAGE
INJURIES TO SOFT TISSUE • PERINEAL TEARS: • TREATMENT: • SHOULD REPAIR IMMEDIATELY FOLLOWNG PLACENTAL DELIVERY • DELAYED BY 24 HRS DELAYED CLOSURE • DIAGNOSE THE DEGREE OF TEAR • GOOD LIGHT, EXPOSURE & ASSISTANCE
INJURIES TO SOFT TISSUE • PERINEAL TEARS: • TREATMENT: • LITHOTOMY POSITION • INCOMPLETE TEAR: CONTINUOUS VAGINAL MUCOSA SUTURE INTERRUPTED TO MUSCLE MATTRESS TO SKIN • COMPLETE TEAR: TAKE FIRST THE RECTAL MUCOSA AND CONVERT TO INCOMPLETE TEAR
INJURIES TO SOFT TISSUE • AFTER CARE: LOW RESIDUE DIET STOOL SOFTNER SEITZ BATH BD ORAL ANTIBIOTICS: ANAEROBIC ANALGESICS
INJURIES TO SOFT TISSUE • VAGINAL LACERATION: • FORCEPS DELIVERIES OR BREECH EXTRACTIONS • OBSTRUCTED LABOUR • TREATMENT: MINOR TEAR: NO SUTURING MAJOR LACERATION: REPAIR USING ABSORABL SUTURE
INJURIES TO SOFT TISSUE • CERVICAL LACERATION: • MINOR INJURY OCCUR IN ALL CASES • DEEP TEARS ARE ALWAYS PREVENTABLE • IDENTIFY AFTER DELIVERY AS PPH • CAUSES: • RAPID DELIVERY OF FETUS • ASSISTED DELIVERIES • RIGID CERVIX
INJURIES TO SOFT TISSUE • CERVICAL LACERATION: • SEQUELAE: • INFECTION, PERSISTENT CERVISITIS • EXTENSIVE SCARRING • STERILITY • REPEATED ABORTION • PREMATURE LABOUR • DYSTOCIA
INJURIES TO SOFT TISSUE • CERVICAL LACERATION: • TREATMENT: MINOR TEAR: NO TREATMENT MAJOR TEAR: INSPECT THE WHOLE CERVIX HOLD THE TORN END WITH SPONGE HOLDING FORCEPS INTURRUPTED CATGUT SUTURES – VERTICAL MATTRESS SUTURE
INJURIES TO SOFT TISSUE • RUPTURE OF UTERUS: • DISRUPTION IN THE CONTINUITY OF UTERINE WALL • INCIDENCE: 0.05% (1 IN 2000) • CAUSES: • SPONTANEOUS: CONGENITAL MALFORMMATION, OBSTRUCTED LABOUR, GRAND MULTIPARITY • SCAR RUPTURE: PREVIOUS CS (1-2%), MYOMECTOMY
INJURIES TO SOFT TISSUE • RUPTURE OF UTERUS: • CAUSES: • IATROGENIC: INJUDICIOUS USE OF OXYTOCIN, FORCIBLE ECV/ IPV, FALL OR BLOW OVER THE ABDOMEN, , FORCEPS or BREECH EXTRACTION • TYPES: • INCOMPLETE RUPTURE: PERITONIUM REMAINS INTACT • COMPLETE RUPTURE: SCAR IN UPPER SEGMENT- INVOLVES PERITONIUM
INJURIES TO SOFT TISSUE • RUPTURE OF UTERUS: • DIAGNOSIS: • DURING PREGNANCY: PAIN OVER LOWER ABDOMEN TENDERNESS SUDDEN ABDOMINAL DISTENSION FEATURES OF SHOCK FHS – IRREGULAR OR ABSENT
INJURIES TO SOFT TISSUE • RUPTURE OF UTERUS: • DIAGNOSIS: • DURING LABOUR: BACKGROUND OF PROLONG OBSTRUCTED LABOUR SHOCK, COLLAPSED STATE WEAK & RAPID PULSE, LOW BP FETAL PART EASILY FELT
INJURIES TO SOFT TISSUE • RUPTURE OF UTERUS: • TREATMENT: • RESUSCITATION: 2 WIDE BORE IV CANULA / VENOUS CUT DOWN / CVP IV FLUIDS: RL / HAEMACCEL BLOOD CROSS MATCH & TRANSFUSE MONITOR VITALS, CVP & UO
INJURIES TO SOFT TISSUE • RUPTURE OF UTERUS: • TREATMENT: • LAPAROTOMY: REPAIR: IN CASES OF SCAR RUPTURE WITH CLEAN MARGIN REPAIR & STERILISATION: HYSTERECTOMY: LOW GENERAL CONDITION, GRAND MULTIPARA, MORBID DISTORTION OF ANATOMY, INFECTED CASE
Episiotomy: • Episiotomy is a surgically planned incision on the perineum and the posterior vaginal wall during the second stage of labor. • It is also known as Perineotomy.
Episiotomy • A surgical incision into the perineum between the vagina and anus. • Prior to instrumental delivery (forceps, vacuum) to widen the vagina
Objective of Episotomy: • To enlarge the vaginal introitus so as to facilitate easy and safe delivery of fetus. • To minimize overstretching and rupture of the perineal muscle and fascia. • To reduce the stress and strain on the fetal head(more for premature baby).
Indications: • In rigid/inelastic perineum- primigravida, old perineal scar of episiotomy 2. Anticipated perineal tear- Primi, big baby, face to pubis or face delivery, narrow pubic arch, breech delivery 3. Operative procedure- forcep or vaccum delivery
4.To shorten the second stage- Heart diseases, severe pre-eclampsia or pre-eclampsia, post C/S cases, postmaturity 5. Foetal Interest- foetal distress, premature baby, breech delivery
Timing of episiotomy: Bulging thinned perineum during contraction just prior to crowning is the ideal time
Advantages: A. Maternal – 1.Easy to repair 2.Prevent prolapse 3.Prevent lacerations extending to rectum. 4.Shortening of 2nd stage of labour B. Foetal- 1.Minimise intracranial injuries in premature baby 2. Reduces foetal asphyxia and acidosis
Types: • Mediolateral • Median • Lateral • J- shaped
Following structures are cut from inside – outwards. • a) The posterior vaginal wall • b) The deep and the superficial transverse perineal muscle,the bulbospongiosus and part of the levator ani muscle. • c) The fascia covering the muscle • d) Transverse perineal branches of the pudendal vessels and nerves. • e) The subcutaneous tissue and the skin.
Procedure: • Cleaning and draping • Anesthesia • Incision - Site and timing - Technique • Repair: - Timing and Methods