Download
1 / 46
480 likes | 848 Views
Oxidative stress, danger, and immune diseases. Intro slides Spring 2013 MCB 5255. Reactive Oxygen Species. Molecules or ions formed by the incomplete one-electron reduction of oxygen Include singlet oxygen; superoxides ; peroxides; hydroxyl radical; and hypochlorous acid

E N D
Oxidative stress, danger, and immune diseases Intro slides Spring 2013 MCB 5255
Reactive Oxygen Species • Molecules or ions formed by the incomplete one-electron reduction of oxygen • Include singlet oxygen; superoxides; peroxides; hydroxyl radical; and hypochlorous acid • Contribute to the microbicidal activity of phagocytes, regulation of signal transduction and gene expression, and the oxidative damage to nucleic acids; proteins; and lipids
Formation and Function • In immune function, synthesized by dedicated enzymes in phagocytic cells • Generated for killing engulfed bacteria • Unavoidable byproduct of cellular respiration • Interaction of ionizing radiation with biological molecules
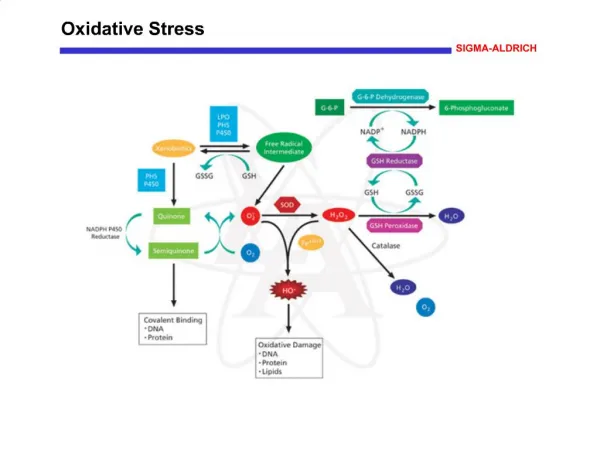
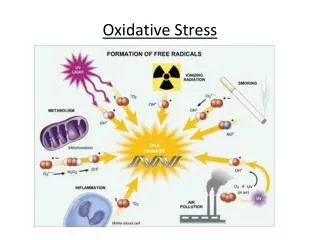
Oxidative Stress SIGMA-ALDRICH
Oxidative Stress Oxidative stress is imposed on cells as a result of one of three factors: 1) an increase in oxidant generation, 2) a decrease in antioxidant protection, or 3) a failure to repair oxidative damage. Cell damage is induced by reactive oxygen species (ROS). ROS are either free radicals, reactive anions containing oxygen atoms, or molecules containing oxygen atoms that can either produce free radicals or are chemically activated by them. Examples are hydroxyl radical, superoxide, hydrogen peroxide, and peroxynitrite. The main source of ROS in vivo is aerobic respiration, although ROS are also produced by peroxisomal ß-oxidation of fatty acids, microsomal cytochrome P450 metabolism of xenobiotic compounds, stimulation of phagocytosis by pathogens or lipopolysaccharides, arginine metabolism, and tissue specific enzymes. Under normal conditions, ROS are cleared from the cell by the action of superoxide dismutase (SOD), catalase, or glutathione (GSH) peroxidase. The main damage to cells results from the ROS-induced alteration of macromolecules such as polyunsaturated fatty acids in membrane lipids, essential proteins, and DNA. Additionally, oxidative stress and ROS have been implicated in disease states, such as Alzheimer’s disease, Parkinson’s disease, cancer, and aging. References Fiers, W., et al., More than one way to die: apoptosis, necrosis and reactive oxygen damage Oncogene., 18, 7719-7730 (1999). Nicholls, D.G., and Budd, S.L., Mitochondria and neuronal survival. Physiol. Rev., 80, 315-360 (2000). Hayes, J.D., et al., Glutathione and glutathione-dependent enzymes represent a co-ordinately regulated defense against oxidative stress. Free Radic. Res., 31, 273-300 (1999).
Oxidative Stress • An imbalance between the production and manifestation of reactive species and the ability to readily detoxify the reactive intermediates • Can cause damage to all components of the cell including proteins, lipids, and DNA • ROS vs RNS • Highly reactive molecules containing oxygen • Peroxides, hydroxyl radicals, superoxide • Highly reactive molecules containing nitrogen • Nitrogen dioxide (·NO2) and dinitrogen trioxide (N2O3)
Antioxidant • A molecule capable of inhibiting the oxidation of other molecules • Oxidation: Loss of electron(s) resulting in an increase in oxidation state • Reduction: Gain of electron(s) resulting in a decrease in oxidation state • Antioxidants are reducing agents • Prevent reactive species from causing damage in the body • Both endogenous and exogenous antioxidants • Endogenous: SOD, glutathione peroxidase, CAT • Exogenous: vitamin C, vitamin E, carotenoids and polyphenols
Defenses against ROS • Antioxidant enzymes such as Superoxide Dismutase and Catalase (2H2O2 -> 2H2O + O2) • Antioxidants such as glutathione GSH • Glu-cys-glytripeptide • Antioxidant proteins such as Metallothionein
Autoimmunity vs Autoimmune disease • Autoimmunity: self recognition by the immune response • Dual recognition (self-MHC plus antigenic peptide) • Jerne network hypothesis • “don’t eat me” signaling (CD47 on erythrocytes) • Autoimmune disease: self recognition with damaging consequences to tissue function • Tissue specific (e.g. T1D) • Systemic (SLE) • “Danger signals”
Hypersensitivities • 4 main hypersensitivities (I-IV) • Type I Anaphalaxis; Immediate; IgE mediated mast cell degranulation • Allergies, atopy • Type II Cytotoxic (IgM and IgG mediated) • Erythroblastosis fetalis, autoimmune hemolytic anemia, pemphigus vulgaris • Type III Immune complex • Serum sickness, RA, • Type IV DTH/contact sensitivity • Contact dermatitis, T1D, RA, Multiple sclerosis
Tolerance • Discrimination of self vs non-self • Central tolerance develops in thymus and bone marrow • (negative selection to eliminate cells reactive with antigens • Present soon after cell expresses antigen receptor • Present at high concentration over long periods of time • Peripheral tolerance/anergy • When cells encounter antigen in the absence of co-stimulatory signals that are usually provided by inflammation • Antigen segregation • Physical barriers to restrict immune cell access • Thyroid, pancreas, intracellular • Regulatory cells that suppress responses • Clonal deletion post activation
Differentiation of autoimmune diseases; organ specific vs systemic • Organ specific • T1D • Multiple sclerosis • Grave’s disease • Autoimmune hemolytic anemia • Myasthenia gravis • Systemic • RA • Scleroderma • SLE
Examples of autoimmune disease that can be transferred across the placenta
Routes to Autoimmune Disease • Pathogens • Cross-reactive antigens/molecular mimicry • Lyme arthritis • Rheumatic fever • Chronic inflammation, immune dysregulation • Disruption of cell/tissue barriers • Sympathetic ophthalmia (granulomatous uveitis) • Toxicants and other stressors • Genetic predisposition • Combinations of the above
http://pubs.acs.org/doi/pdf/10.1021/tx9003787 (see class website for link)
Genes involved in autoimmune disease • Single gene models • Fas, FasL; ALPS (defects in apoptosis, lymphoaccumulation, angergy and SLE-like autoimmune disease) • Mev; viable motheaten, Hcph-1; SHP1 (chronic inflammation) • IPEX immune dysregulation X linked recessive mutation in transcription factor FoxP3; severe allergic inflammation, hemolytic anemia, thrombocytopenia, etc. • Deficiency in CD25 (IL2R); impaired peripheral tolerance • CTLA4 mutation; Graves disease, T1D, etc. • C1q mutation SLE • MHC associations with autoimmune disease (e.g. HLA-B27)
Function of SHP-1 • Negative regulator of signal transduction • growth factor receptors: c-kit, EPO • activation signaling: BCR, TCR, NK activating receptor • SHP-1 inactivates anti-apoptotic signaling molecules in neutrophil proliferation • induces apoptosis in sympathetic neurons
Clinical disease in viable motheaten mice • Anemia • Immunodeficiency • Autoimmunity • Death from acidophilic macrophage pneumonia
Macrophage pneumonia in mev/mev mice +/? mev/mev
Approaches to identifying genes involved in autoimmune disease • GWAS genome wide associational studies • Family studies to identify SNP that track with autoimmune disease • Animal models with mutations in candidate genes • Meta-analysis of data to enlarge patient populations studied for autoimmune disease
Biochemistry of autoimmune disease • Biochemical events that potentiate autoimmunity • events that cause damage to membrane, etc • Reactive oxygen, chronic inflammation • Biochemistry of damaging events associated with autoimmune disease • Reactive oxygen, chronic inflammation
Figure 1. Pathogenesis of diabetic microvascular complications. This schematic proposes that the development of microvascularcomplications begins early in the course of diabetes, well before clinical diabetes is detected. Certain genetic characteristicsor polymorphisms (Apo E4, Aldose reductase, ACE) may increase individual predisposition for development of microvascularcomplications of diabetes [30,31], whereas other genetic factors, such as the toll receptor, are protective and decreasepredisposition. The various inflammatory mediators listed under the heading of inflammation cause direct cellular injury andinitiate the cycle of functional and progressive pathologic changes, which ultimately manifest as microvascular complications[13,15–18,21]. As the disease progresses, lipotoxicity [28], glucotoxicity [42,43], and epigenetic factors further contribute to thefunctional and pathologic changes. Intervention with insulin or insulin sensitizers, particularly in the early stages of pathogenesis,can counteract inflammatory changes, control glycemia, prevent formation of advanced glycation end products, and ameliorateoxidative-stress-induced overactivation of poly adenosine diphosphate ribose polymerase (PARP), with the potential to changethe natural history of microvascular complications [29,37]. ApoE4 = Apolipoprotein E4; ACE = Angiotensin-converting enzyme;PKCβ = Protein kinase C beta; IL-6 = Interleukin-6; TNFα = Tumor necrosis factor alpha; NFκ B = Nuclear factor kappa B. Adaptedwith permission from Vinik A, Mehrbyan A. Diabetic neuropathies. Med Clin North Am 2004; 88: 947–999 http://onlinelibrary.wiley.com/doi/10.1002/dmrr.530/pdf Diabetes Metab Res Rev 2005; 21: 85–90.
http://nihroadmap.nih.gov/epigenomics/epigeneticmechanisms.asphttp://nihroadmap.nih.gov/epigenomics/epigeneticmechanisms.asp
Histone modifications http://www.nature.com/nsmb/journal/v14/n11/images/nsmb1337-F1.gif
http://www.cellsignal.com/reference/pathway/Histone_Methylation.htmlhttp://www.cellsignal.com/reference/pathway/Histone_Methylation.html
Diabetes is not the only context in which histone methylation is potentially important. For example: • H3K4me3 demethylases : link between histone modifications and XLMR. • X-linked mental retardation (XLMR) gene SMCX (JARID1C), • which encodes a JmjC-domain protein, reversed H3K4me3 to • di- and mono- but not unmethylated products//Cell 2007 • The putative oncogene GASC1 demethylates tri- and dimethylated • lysine 9 on histone H3//Nature (2006) 442: 307-11. • Sustained JNK1 activation is associated with altered histone H3 • methylations in human liver cancer. //J Hepatol. 2009, 50: 323-33 • Perturbation of epigenetic status by toxicants// • Toxicology LettersVolume 149, Issues 1-3, 1 April 2004, Pages 51-58
Type 1 diabetes, which was previously called insulin-dependent diabetes mellitus (IDDM) or juvenile-onset diabetes, may account for 5% to 10% of all diagnosed cases of diabetes. Type 2 diabetes, which was previously called non-insulin-dependent diabetes mellitus (NIDDM) or adult-onset diabetes, may account for about 90% to 95% of all diagnosed cases of diabetes. Gestational diabetes is a type of diabetes that only pregnant women get. If not treated, it can cause problems for mothers and babies. Gestational diabetes develops in 2% to 5% of all pregnancies but usually disappears when a pregnancy is over. Other specific types of diabetes resulting from specific genetic syndromes, surgery, drugs, malnutrition, infections, and other illnesses may account for 1% to 2% of all diagnosed cases of diabetes. http://www.cdc.gov/diabetes/consumer/learn.htm
Rate of new cases of type 1 and type 2 diabetes among youth aged <20 years, by race/ethnicity, 2002–2003 <10 years 10–19 years CDC. National Diabetes Fact Sheet, 2007. Source: SEARCH for Diabetes in Youth Study NHW=Non-Hispanic whites; AA=African Americans; H=Hispanics; API=Asians/Pacific Islanders; AI=American Indians
Humanized mouse models Humanized mouse models to study human diseases Brehm et al.
Your presentations • Each presentation is ~1 hour • Spend first 20 minutes or so describing the fundamental information: what do we need to know to understand the papers you have assigned? How does this presentation fit into the course main topic? • Divide the second 30 minutes into discussions of each of the two contemporary papers that you assigned to the class at the previous class period
Grantsmanship: NIH Steps to the NIH grant application process http://funding.niaid.nih.gov/researchfunding/grant/pages/applying.aspx NIH electronic grant forms http://grants.nih.gov/grants/funding/424/index.htm Examples of outstanding titles and abstacts http://funding.niaid.nih.gov/researchfunding/grant/pages/titleabs.aspx Search engine for currently funded grants http://projectreporter.nih.gov/reporter.cfm Tongue-in-cheek": how to fail in grant writing http://chronicle.com/article/How-to-Fail-in-Grant-Writing/125620/
Discussion points to include • What is the fundamental hypothesis that is being tested? • What techniques did they use that we have to understand to evaluate the data? • What are the most important figures/data sets that we should discuss? • Are there alternative interpretations of their data? • What conclusions did they reach? • What new questions do they open up with their results?
Grant application • Hypothesis and ONE specific aim are due March 5 to be discussed on March 6th • Grant is due May 5 (first day of exam period) by 5pm (hard copy plus electronic e-mailed file please)
Grant format: • TEXT: • Hypothesis and specific aim (0.5 page) • Background and Significance (3-4 pages) • What do we know about the system? • What makes this hypothesis tenable? • How is the approach you propose innovative? • Research designs and Experimental approach (4-5 pages) • Rationale • Experimental design and methods • Anticipated outcomes • Potential pitfalls and alternative approaches • We will talk about NIH forms later in the semester
Inflammatory Bowel Disease • Include: • Crohn’s Disease • Ulcerative Colitis • Autoimmune disease—idiopathic • Current treatments: • Treat symptoms, reduce frequency • Surgical resectioning
Effects of IBD • Severe inflammation, perforation of intestinal epithelium • Strictures, fistulae, toxic megacolon, perianal disease • Arthritis common, may be unrelated • Increased risk of cancer, infection
Oxidative Stress in Autoimmune Disease • Excessive oxidative stress is thought to have an important role in the pathogenesis of many autoimmune diseases • Enhances inflammation, induce apoptotic cell death, disrupt signal pathways • Seen in diseases such as: • RA • SLE • IBD • MS