Download
1 / 141
1.42k likes | 1.48k Views
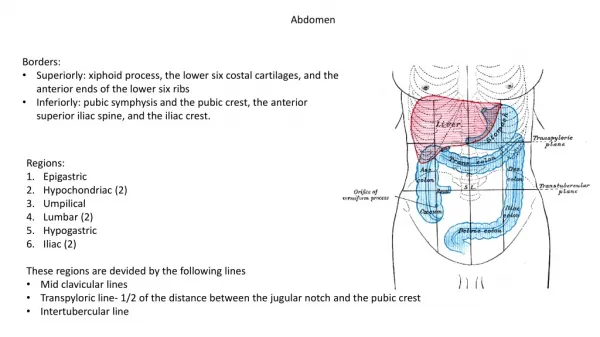
ABDOMEN. Infection. Infection:. Appendicitis Diverticulitis Perinephric Abscess Renal Abscess. APPENDICITIS. Description:. Appendicitis is the inflammation of the vermiform appendix due to an obstruction. Appendicitis is the most common acute surgical condition of the abdomen. Etiology:.

E N D
ABDOMEN Infection
Infection: Appendicitis Diverticulitis Perinephric Abscess Renal Abscess
Description: • Appendicitis is the inflammation of the vermiform appendix due to an obstruction. Appendicitis is the most common acute surgical condition of the abdomen.
Etiology: • Obstruction of the vermiform appendix.
Epidemiology: • Appendicitis can occur at any age and affects males and females equally.
Signs and Symptoms: • Patient may present with abdominal pain or tenderness in the right lower quadrant (McBurney point), anorexia, nausea and vomiting, and constipation.
Imaging Characteristics: • CT examination may be performed either with or without IV contrast. No oral contrast is needed. CT • Dilated, fluid-filled appendix. • May present with a calcified appendicolith. • Ring-like enhancement with contrast. • Associated with periappendiceal inflammation or abscess.
Treatment: • Immediate surgical intervention (appendectomy) is required.
Prognosis: • Usually uncomplicated course of recovery in non-ruptured appendicitis. If the appendix ruptures, there is a variable degree of morbidity and mortality based on the age of the patient.
Figure 1. Appendicitis Axial CECT (A) shows an enlarged rim enhancing appendix in the right lower quadrant of the abdomen near the cecum with adjacent fat stranding consistent with acute appendicitis. Coronal MPR (B) shows an enlarged enhancing appendix with an appendicolith (arrow).
Description: • Diverticulitis is a complication of diverticulosis. Diverticulitis is an abscess or inflammation initiated by the rupture of the diverticula into the pericolic fat.
Etiology: • Diverticulitis is a secondary complication to ruptured diverticula.
Epidemiology: • Diverticulosis rarely affects those younger than 40. About 40% to 50% of the general population is affected by the time they reach their sixth to eighth decade of life.
Signs and Symptoms: • Pain is most commonly seen in the left lower quadrant. The patient usually experience either diarrhea or constipation. When considering diverticulitis, in addition to the above, patients will experience fever with chills, anorexia, nausea and vomiting, and tenderness in the left lower quadrant.
Imaging Characteristics: CT • Early signs of diverticulitis include wispy, streaky densities in the pericolic fat, and a slight thickening of the colon wall. • Severe cases of diverticulitis may demonstrate pericolic abscesses.
Treatment: • Usually treated with IV antibiotics. Abscess may require CT-guided drainage or surgical intervention.
Prognosis: • With early detection and treatment the patient should experience a good recovery.
Figure 1. Diverticulitis Axial CECT with positive oral contrast shows a moderate amount of fat stranding adjacent to the descending colon on the left due to diverticulitis.
Figure 2. Diverticulitis Axial CECT shows multiple diverticula arising from the sigmoid colon, several of which are marked with arrowheads. There is no evidence of acute diverticulitis.
Description: • A perinephric abscess is a collection of pus within a fatty tissue around the kidney.
Etiology: • Its results from a bacterial infection such as E coli and Proteus, and Staphylococcus in a few cases.
Epidemiology: • Perinephric abscesses usually arise froma preexisting renal inflammatory disease. However, they may occur as a result of complication of surgery and trauma, or spread from other organs.
Signs and Symptoms: • Patients will present with flank or back pain, fever, nausea and vomiting, malaise, and painy urination
Imaging Characteristics: CT • Abscess appears with lower than normal attenuation (hypodense) values when compared to normal parenchyma. • Rim enhancement of the abscess occurs with administration of IV contrast. • Stranding densities in the perirenal fat and thickening of the renal fascia. • Gas pockets may be seen within the abscess. • Contrast-enhanced CT is the modality of choice for the diagnosis.
Treatment: • Intravenous administration of antibiotics and percutaneous catheter drainage. Surgery is rarely needed.
Prognosis: • Generally good with early diagnosis and treatment.
Figure 1. Left Perinephric Abscess Contrast CT of the abdomen shows a large fluid collection (thick arrow) around the left kidney (asterisk). Note: There are gas bubbles within the fluid collection (small arrows).
Figure 2 Perinephric Abscess CECT shows a rim-enhancing fluid collection adjacent to the right kidney which also contains a few foci of air consistent with a perinephric abscess.
Description: • A renal abscess is a collection of pus within the parenchyma of the kidney.
Etiology: • Results from a bacterial infection.
Epidemiology: • Most renal abscesses are the result of an ascending infection and are usually due to gram-negative urinary pathogens, in particular E-coli. To a lesser degree, renal abscesses may be due to a complication from surgery, trauma, spread from other organs, or lymphatic spread.
Signs and Symptoms: • Patients will present with flank or back pain, fever, nausea and vomiting, malaise, and painful urination.
Imaging Characteristics: CT • Abscess appears with lower than normal attenuation (hypodense) values when compared to normal parenchyma. • Rim enhancement of the abscess occurs with administration of IV contrast. • Stranding densities in the perirenal fat and thickening of the renal fascia. • Gas pockets may be seen within the abscess. • Contrast-enhanced CT is the modality of choice for the diagnosis.
Treatment: • Intravenous administration of antibiotics and percutaneous catheter drainage. Surgery is rarely needed.
Prognosis: • Generally good with early diagnosis and treatment.
Figure 1. Left Renal Abscess CT of the abdomen with IV contrast demonstrates a round low-density mass in the upper pole of the left kidney. Ultrasound showed this mass to be complex. Combination of these findings in a patient with flank pain, fever, and leukocytosis is consistent with a renal abscess.
Figure 2. Renal Abscess CT-guided needle aspiration of a cystic mass in the upper pole of the left kidney yielded pus. The aspirating needle is within the abscess. This abscess was successfully treated with catheter drainage and antibiotics.
Trauma ABDOMEN
Trauma: Liver Laceration Renal Laceration Splenic Laceration
Description: • Lacerations to the liver can occur as a result of blunt or penetrating abdominal trauma, as a complication of surgery, or an interventional procedure.
Etiology: • A laceration to the liver usually results from an injury, such a blunt or penetrating abdominal trauma. However, complication of surgery or an interventional procedure can also result in a laceration-type injury.
Epidemiology: • Trauma to the abdomen results in approximately 10% of all traumatic deaths. Many of these injuries occur as secondary injuries as a result of high-speed motor vehicle accidents.
Signs and Symptoms: • Abdominal pain resulting from the blunt trauma or an open wound occurring from a penetrating injury. The patient may experience hypovolemic shock that is caused from an inadequate blood volume.
Imaging Characteristics: CT • A noncontrast study may not reveal the injury. • Contrast enhancement will assist in demonstrating the laceration as a hypodense area. • May show subcapsular hematoma. • May show hemoperitoneum. • CT with IV contrast is the imaging modality of choice in the evaluation of abdominal trauma.
Treatment: • Emergency surgical intervention may be required to repair the laceration of the liver in hemodynamically unstable patients. Stable patients with small lacerations can be treated conservatively.