Download
1 / 65
680 likes | 767 Views
ABDOMEN. Anatomical landmark in clinical exploration of the abdomen. What is normal?. Bony landmarks. Lower ribs Spine Iliac bone Inguinal ligament Pubic bone Sacrum – pelvic aperture. Anatomic landmarks. Xifoid apendix Costal margins Spina iliaca antero-superior Simphisis pubis

E N D
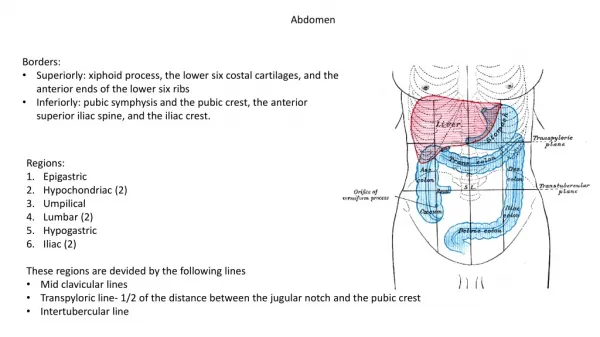
Bony landmarks • Lower ribs • Spine • Iliac bone • Inguinal ligament • Pubic bone • Sacrum – pelvic aperture
Anatomic landmarks • Xifoid apendix • Costal margins • Spina iliaca antero-superior • Simphisis pubis • Umbilical scar
Topography of abdominal wall • Vertical lines • Midline between pubis and antero-superior iliac spine • Horizontal lines • Through both iliac spines • Subcostal (lower most part of costal margin)
Antero-lateral wall. Essentials of anatomy. I • Skin • Subcutaneous tissue • Vascular and nervous structures • Umbilical scar • Inguinal arrea
Antero-lateral wall. Essentials of anatomy II • Muscles and corresponding fascia (internal and external oblique, transversalis and rectus abdomini) • Linea alba • Posterior aspect of the inguinal region • Umbilical region • Vessels and nerves
Posterior wall. Essentials of anatomy • Diaphragm • Diaphragmatic communications • Muscles of the lumber region • Muscles of the pelvic diaphragm
Inguinal region • Skin projection of the region (triangle) • Inguinal ligament • Lateral aspect of rectus abdomini • Perpendicular through the middle of ilio-pubic line
Examination of the abdomenThe abdominal wall • Inspection • Palpation • Percussion • Auscultation
Inspection • Shape • Asymmetry • Changes in decubitus and standing • Scars • Cutaneous changes • Vascular pattern
Palpation - superficial • The structure of the abdominal wall • Sensibility • Cutaneous reflexes • Subcutaneous tissue • Weak points and areas • Muscular structures • Check muscle position within the structures
Good light Relaxed patient Correct exposure. Whole abdomen to the level of symphisis and inguinal region Protect the genital areas Decubitus + pillow Arms close to the body Ask patient for painful areas and examine them later Warm hands Avoid sudden movements Distract his attention if anxious Follow his reactions – face changes Clinical examination of the abdomen
Methods • Anamnesis • Inspection • Palpation • Percution • Auscultation • Rectal and vaginal examination
History taking • PAIN • Onset and time changes • Location • How significant • Radiation of pain • Association with other symptoms
Types of abdominal pain • Hollow organs • Paroxistic crampy pain • Difficult to pinpoint • Associated with peristaltic movement • Pacient is agitated – would not find a relaxed position • Perioneal inflamation • Constant or steadily increasing pain • Well circumscribed • Patient will be reluctant to move as it increases pain
Radiated pain • Billiary colic • Duodenal ulcer • Renal pain • Genital originated pain
Essentials of anamnesis • Nausea, vomiting, diarrhea, constipation • Stool – melena, blood, • Vomiting – blood, digested blood • Urinary symptoms : frequency, discomfort • Weight loss • Sexual history • Sexual activity, contraceptive pills, last cycle • Any fertile women may be pregnant • Pregnancy test if in doubt
Skin Venous pattern Umbilical scar Shape of abdomen Peristaltic movement Pulsations Mobility during cough or respiration INSPECTION
AUSCULTATION • Preferable before palpation – stimulates movements • Listen for sounds produced by bowels • Vascular abnormal sounds (stenotic vessels)
First orientation – “in cross” in four quadrant Map of the abdomen Generalized/localized meteorism Dull area localized +/- movable Signs of peritoneal irritation PERCUSSION
PALPATION • Essential and the most important • One or two hands are used for deep palpation depending mostly on muscular tonus • Systematic, avoid very painful areas at the beginning • After a screening examination – characterize different organs which are accessible • Sudden decompression
Rectal examination • Sensible area • Put yourself (only in theory…) in his/her place • He/she should trust you • A special room – respect his/her dignity
Rectal examination • Lateral decubitus or in all fours • Explain what you do. It is not painful nor pleasant • All you need is a glove and lubricant
Rectal examination • Inspection: • Eritematous lesions • Incontinence for feaces • Scars • Fistula – puss • Tumors • Ulcerations • Fissura in ano
Rectal examination • Palpation: • Sphyncter tonus • Fissura in ano • Prostate • Tumors • Rectal content • Cervix and uterus • Peritoneal “Coul de sac” or Douglas pouch • Bimanual examination • Look for faces aspect on you glove
Inspection • Volume • Uniform distension in ascites • Asymmetric distension in tumors • Venous collateral circulation
Inspection • Umbilical hernia • Spider hemangioma • Gynecomastia • Rinofima
More often unhelpful Before ascites there is a period with paretic distension with dimished intestinal sounds Large tumors with lare tributaries – arterial murmurs Acoustic finding of liver edge Auscultation
Percussion • Evaluate the area of liver dullness • If significantly increased you need to find both edges • In general the liver is underestimated
Percussion • Meteorism before ascites • Movable dullness • Iceberg sign • Wave sign • Prehepatic tympanism • Sdr. Chilaiditi • Pneumoperitoneum • Situs inversus
Palpation • Inferior limit of the liver • Limits • Morphologic aspect • Sensibility • Tumors • charcaterize
Rectal examination • Faeces with melena aspects • Fresh • Old • Large volume internal hemorrhoids (portal hypertension) • Metastasis in the Douglas pouch
Inspection • Changes determined by anemia or hematological diseases • Abdominal deformities • Peritoneal irritation in trauma with blood in peritoneum
Percussion – dull area of the spleen - movable dullness – liquid in peritoneum