Download
1 / 56
570 likes | 838 Views
ĐẠI CƯƠNG VỀ HỆ ĐƠN NHÂN-THỰC BÀO & TẾ BÀO DENDRITIC. TẾ BÀO MONOCYTE & THỰC BÀO Nguồn gốc Từ tủy xương :tế bào gốc biệt hoá granulocyte –macrophage colony forming unit (GM-CFU) →promonocyte →monocyte:vào mạch máu Tại máu ngoại biên :monocyte (20-40g) → mô :nhiều tên

E N D
ĐẠI CƯƠNG VỀ HỆ ĐƠN NHÂN-THỰC BÀO & TẾ BÀO DENDRITIC • TẾ BÀO MONOCYTE & THỰC BÀO • Nguồn gốc • Từ tủy xương :tế bào gốc biệt hoá granulocyte –macrophage colony forming unit (GM-CFU)→promonocyte →monocyte:vào mạch máu • Tại máu ngoại biên :monocyte (20-40g) → mô :nhiều tên • Nhiệm vụ;tiêu hoá và giết các vi sinh vật lạ và trình diện kháng nguyên cho tế bào miễn dịch • Phân biệt monocyte và macrophage
BỆNH HISTIOCYTOSIS ĐẠI CƯƠNG Hệ tế bào Monocyte và Macrophage Hệ tế bào Dendritic HỘI CHỨNG HISTIOCYTOSIS Đại cương về hội chứng Histiocytosis Hemophagocytic Lymphohistiocytosis Langerhans Cell Histiocytosis Malignant Histiocytosis Syndrome
ĐẠI CƯƠNG VỀ HỆ ĐƠN NHÂN-THỰC BÀO & TẾ BÀO DENDRITIC
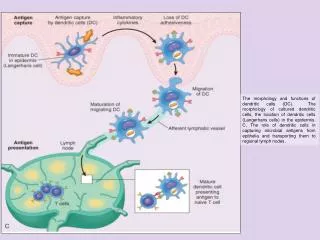
TẾ BÀO DENDRITIC • Nguồn gốc:myeloid dendritic cells & lymphoid dendritic cell, • Nhiệm vụ:trình diện kháng nguyên cho tế bào T và B • Phân biệt tế bào dendritic
HỘI CHỨNG HISTIOCYTOSIS • ĐẠI CƯƠNG • Lịch sử:1987 ,hội Histiocytosis :LS+ Bệnh học+ Miễn dịch học • Nguyên tắc phân loại:hình dạng,hoá học,dấu ấn bề mặt
TIÊU CHUẨN CHẦN ĐOÁN HCTB • Chẩn đoán phân tử xác định • Có 5/8 đặc điểm • Tiêu chuẩn đầu tiên • Lâm sàng:sốt .38.50 C và > 7 ngày • Xét nghiệm: • giảm 2/ 3 dòng :Hb <9g/dL,PN <1000/mm3,TC < 100000/mm3. • 1/2 tiêu chuẩn :hypofibrinogen <150mg/dL,hypertriglyceride > 3mmol/L • Giải phẩu bệnh:Hemophagocytosis trong tuỷ,hạch,lách ,gan.Không tế bào ác tính. • Tiêu chuẩn bổ sung: • Natural killer giảm hoạt lực • Ferritin ≥ 500 microgram/L • CD25 hoà tan (IL2 receptor) ≥ 2400U/L • Ngoài ra các tiêu chuẩn hỗ trợ : • Lâm sàng:TC não màng não,hạch to,vàng da,phát ban,men gan ,đạm máu,natri máu,VLDL ,HDL . • Dịch nảo tuỷ:monocyte tăng,protein tăng
New diagnostic guidelines for HLH(HLH-04) The diagnosis of HLH can be established if either one of the 1 or 2 below is fulfilled- ① A molecular diagnosis consistent with hereditary HLH. ② Clinical diagnostic criteria fulfilled for 5 out of the 8 criteria below. Clinical 1 Fever 2 Splenomegaly Laboratory 3 Cytopenia 4 Hyper-triglyceridemia and/or hypo- fibrinogenemia Histopathologic 5 Hemophagocytosis Biological markers 6 Low or absent NK cell activity 7 Ferritin ≧500 μg/L 8 sIL-2R ≧ 2400 U/ml
THỂ DI TRUYỀN HEMOPHAGOCYTIC LYMPHOHISTIOCYTOSIS • = familial hemophagocytic lymphohistiocytosis (FLH) • ĐẠI CƯƠNG :2/1M/năm (< 15 tuổi ), < 1 tuổi 80% • SINH LÝ BỆNH :di truyền NST lặn ,có thay đổi 10q21-22 (20-30%) ; 17q 25; Xq25. • TCLS: sốt, chậm lớn,gan lách to,thiếu máu.Tổn thương hạch,phổi,tim,hệ TKTU,xương mô mềm,hệ tiêu hoá. • CLS:giảm BChạt +Bc atypic,đơn nhân bất thường,chức năng bị thay đổi :tăng transaminase,tăng triglyceride,cholesterol. • CHẨN ĐOÁN: • Tuổi thường nhỏ (< 3 tháng); • Tiền sử anh chị ruột bị tử vong sớm. • Chẩn đoán giải phẩu bệnh: chọc tủy, sinh thiết hạch ,gan,lách,thy mus : histiocyte qua khảo sát dấu ấn tế bào dương tính :S-100,CD11c,CD 14,CD35,CD68.Fc receptor,IL-2.
SINH LY BỆNH HCTB DI TRUYỀN • Tần suất :1,2/1.000.000 trẻ /năm • Đặc điểm:di truyền kiểu lặn nên tiền sữ GĐ có thể bình thường. • Hậu qủa miễn dịch:giảm hoạt lực CD8,NK,tăng IL-2. • Di truyền NST lặn ,có thay đổi • Mutation:Gen:FHL1 (9q21.3-32) • Mutation Perforin gene(10q21) :20-40% ,giảm NK-T cell cytotoxicity (FHL 2) • Mutation Munc gene:( 17q25) :giảm cytolytic granules exocytosis .(FHL3) • FHL4: gen tạo ra syntaxin 11(6q,24) hạt tiêu bào • Mutation gen SAP hay SH2-DIA (Xq25) là gen tạo ra protein dẫn truyền trong LT và NK.
Hypercytokinemia causes fatal opportunistic infections, hemorrhages, and multiple organ dysfunction
APC (virus-infected cell) HLH-causing dis. T-cell killing Deficient activation(SAP mutation) XLP Activation Impairment of LG release (AP-3,Lyst,Rab27a,Munc13-4,STX11) Hermansky-Pudlack, Chediak-Higashi, Griscelli, FHL3, FHL4 Cytokine production LG release Lack of active perforin FHL2 Activation of macrophages
CTL secretory lysosomes Golgi complex Vesicle docking and fusion SL N AP-3 CHS1 Target (APC) N RabGGTase Microtubule-dependent movement AP-3; Hermansky-Pudlak syndrome II CHS1; Chediak-Higashi syndrome, RabGGTase; defect in CTL killing Perforin; FHL2 Rab27a; Griscelli disease type 2 Syntaxin 11: FHL4 Munc13-4; FHL3 VAMP SNAP-23
Molecular abnormalities developing FHL diseaseabnormal molecules (chr. locus) FHL1unknown(9q21.3-22) FHL2 perforin (10q21-2) FHL3 munc13-4 (17q25) FHL4 syntaxin 11(6q24)
Hokkaido ■ Aomori ■ Nagano Hiroshima Kyoto Fukuoka ● ● ● Saga Ibaraki ●●● ●● ■ ● ■ ■ ●● ● ● Nagasaki ■■■■ Osaka Okinawa Yokohama ● Kagawa Kagoshima Geographic origins of the FHL patients in Japan Open : perforin gene mutation positive Closed : perforin gene mutation negative ○ : family history(FH) positive □ : NK activity deficient (FH negative or unknown) Open : perforin gene mutation positive Closed : perforin gene mutation negative ○ : family history(FH) positive □ : NK activity deficient (FH negative or unknown) Sea of Japan Sea of Japan Sea of Japan FHL2 : ● FHL3:■ Sea of Japan Sea of Japan Pacific Ocean Pacific Ocean Pacific Ocean Kyoto Osaka Kyoto Osaka Kyoto Osaka Pacific Ocean Pacific Ocean Kyoto Osaka Kyoto Osaka Fukuoka Fukuoka Fukuoka ■ ○○ ■ ○○ ■ ○○ ○ ○ ○ ■■● □◯ ■■● □◯ ■■● □◯ Saga Saga Saga ● ● ● Ibaraki Ibaraki Ibaraki Fukuoka Fukuoka ■○ ○○○ ■○ ○○○ ■○ ○○○ ● ● ● ■ ■ ■ ■ ○○ ■ ○○ □ □ □ ○ ○ ○ ○ ○ Nagasaki Nagasaki ■■● □◯ ■■● □◯ Saga Saga ● ● Ibaraki Ibaraki ■○ ○○○ ■○ ○○○ ● ● ■ ■ □ □ ○ ○ Nagasaki
What we have learned from FHL study: 1. FHL2, FHL3 and FHL4 are able to be diagnosed molecularly. 2. No FHL4 is detectable in Japan, which has been found mostly in Turkey (Kurdish). 3. Responsible gene(s) remain unknown in about half of the FHL cases. 4. Late onset cases of FHL (> 5yrs, up to 62yrs) have been found, thus the development of FHL is not limited in infancy. 5. The major cause of primary HLH, such as FHL、CHS, GS, resides in the defect in lysosomal secretory vesicles in NK cell/ cytotoxic T cell.
Residual NK/CTL activity Gene mutations Onset of HLH missense/missense or missense/nonsense Late onset (>5yrs as late as in adult) or undeveloped yes FHL (FHL2, FHL3) Early onset (<2yrs), with progressive disease no nonsense/ nonsense Missense; single nucleotide change Nonsense (disruptive); premature stop codon, or sequence frameshift
Fatal HLH LCMV (lymphocytic choriomeningitis virus) -infected no infection Perforin knock-out mouse No HLH, alive
HCTB THỨ PHÁT • Nguyên nhân nhiễm trùng • Virus:EBV ,CMV,Dengue,Adenovirus,Herpes simplex,HIV,Parvovirus • Vi trùng:Babesia microti,Bruscella abortus,Enteric grame -,Hib ,Mycoplasma pneumonia,Staphylococcus aureus,Streptococcus pneumo • Mycobacter tuberculosis,Rickett siella • Vi nấm:Candida albican,Crytococcus neoformant,Histoplasma capsultum • Ký sinh trùng:Leishmania donovani • Nguyên nhân miễn dịch ; bệnh tự miễn, viêm đa khớp thể thiếu niên • Nguyên nhân bệnh máu ác tính : lymphoma, bạch cầu cấp
Primary (hereditary) Secondary ( )
Non-EBV infection-associated, or collagen disease-associated HLH FHL T-LAHS HLH B-LAHS EBV-HLH sJIA-MAS 0 2 10 20 50 年齢(yrs)
HCTB THỨ PHÁT • LÂM SÀNG: sốt kéo dài,đau cơ,mệt mỏi,gan lách hạch to. • XÉT NGHIỆM • CTM :giảm ba dòng,rối loạn đông máu,rối loạn chức năng gan • Tuỷ đồ :GĐ sớm tăng sinh tế bào ,GĐ muộn :nghèo +Histiocyte đang thực bào • XN MÔ HỌC :nhiều tế bào histiocytosis tại gan ,lách • ĐiỀU TRỊ : • Không điêu trị đặc hiệu . • Điều trị bệnh nền là chính. Cần lưu ý các bệnh nền :EBV ,CMV • .Khi có chứng cớ nhiễm EBV thì dùng Acyclovir .
CƠ CHẾ SINH BỆNH HCTB SAU NHIỄM TRÙNG • Tác nhân nhiễm trùng kích thích hệ thống miễn dịch và hoạt động giữa tế bào điều hoà miễn dịch đối với sự phục hồi của ký chủ.Khi có sự rối loạn điều hoà miễn dịch sẽ đưa đến sự đáp ứng không đồng bộ chống lại tác nhân gây bệnh.Sự kích hoạt LT quá mức sẽ đưa đến sự tăng sinh và hoạt hoá mô bào.
ĐiỀU TRỊ HCTB MÁU • ĐIỀU TRỊ • ĐIỀU TRỊ BAN ĐẦU • Thuốc ức chế miễn dịch:Etoposide+Dexamethasone+CyclosporinA • Thuốc chống nhiễm trùng:Cotrimoxazole,chống nấm ,kháng virus. • Khi có dấu hiệu thần kinh,hoặc dịch não tuỷ sau 2 tuần không cải thiện. • Immunoglobulin:0,5g/kg/ 4 tuần. • Thời gian điều trị :8 tuần • ĐIỀU TRỊ DUY TRÌ • Mục tiêu:không cho bệnh tái hoạt động • Thuốc : Etoposide+Dexamethasone+Cyclosporin A • Truyền immunoglobuline 0,5g/kg/4 tuần • Thời gian điều trị :9-40 tuần • ĐIỀU TRỊ CŨNG CỐ • Mục tiêu:không cho bệnh tái phát • Biện pháp ĐT :ghép tuỷ hay kéo dài điều trị duy trì, tăng ĐT Etoposide+Cycl • Hoặc Cyclosporine A+Dexa cách khoảng,tiếp tục Dexa hay Cyclosporine • FHL đáp ứng tốt với etoposide và dexa,Ghép tuỷ là biện pháp hữ hiệu nhất.
Concept of HLH treatment 1. Prompt control of hypercytokinemic condition 2. Care of organ dysfunction, esp. of hemorrhagic diathesis, pulmonary/ renal failure 3. Identification of infectious agent(s) as early as possible. 4. Differentiation of primary and secondary HLH
Therapeutic algorithm EBV-HLH 8 weeks