Download
1 / 50
540 likes | 1.13k Views
CMR of Non-ischemic Dilated and Restrictive Cardiomyopathies. Frederick L. Ruberg, MD Director, Advanced Cardiac Imaging Program Section of Cardiology, Department of Medicine Department of Radiology Boston University School of Medicine Boston Medical Center March 2, 2009.

E N D
CMR of Non-ischemic Dilated and Restrictive Cardiomyopathies Frederick L. Ruberg, MD Director, Advanced Cardiac Imaging Program Section of Cardiology, Department of Medicine Department of Radiology Boston University School of Medicine Boston Medical Center March 2, 2009
Utility of CMR in LV systolic dysfunction • Diagnosis • Ischemic vs. Non-ischemic • Etiology • Prognosis • Functional recovery with treatment • Morbidity and mortality
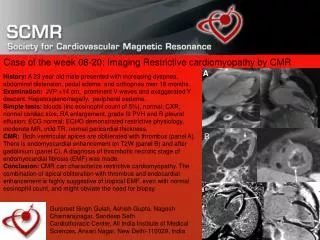
Case Presentation • 58 year old woman with class II-III HF symptoms referred for echo
Why obtain CMR next? • Precise quantification of LV and RV function and volumes from cine images • Permit detection of improvement or decrement with treatment • Quantification of associated valvular regurgitation • Visualization of fibrosis or infarction (DE/LGE) • Pattern of DE important to differentiate etiology • Afford predictors of recovery • Afford predictors of CRT efficacy
LGE Imaging: Initially for scar Kim RJ et al., Circulation 1999
Fibrosis Imaging by DE/LGE • Imaging 10-20 min after gadolinium (0.1 to 0.2 mmol/kg) • Retained contrast in regions of fibrosis or infarction • No contrast in normal myocardium Marholdt EHJ 2005
Ischemic DE Pattern by CMR Marholdt EHJ 2005
Differentiation of Ischemic vs. Non-ischemic CMP • 90 patients with CHF and LV dysfunction obtained cardiac cath and CMR • 70% without CAD by cath • 59% no DE • 28% mid-wall DE • 13% sub-endocardial DE (mis-assigned) • 30% with CAD and history of MI • 100% with sub-endocardial DE McCrohon et al. Circ 2003
Ischemic vs. non-ischemic Ischemic Non-ischemic McCrohon et al. Circ 2003
Case Example – Ischemic or Non- • 35 year old male with severe LV dysfunction • TSH > 120
Mid-wall enhancement • Not subendocardial, does not follow infarction pattern • Most frequently septal • Lower signal intensity vs. MI • Etiology and significance is controversial
Mid-wall enhancement: Morbidity and Mortality • 101 patients with dilated CMR underwent CMR and were followed for 685 days • 35% had mid-wall enhancement • Increased risk of death or hospitalization (OR 3.4) • No difference in mortality • Increased likelihood of SCD/VT (OR 5.2) • Persisted after correcting for LVEF Assomoul et al. JACC 2006
Mid-wall enhancement: Morbidity and Mortality Assomoul et al. JACC 2006
Histologic correlate of mid-wall Assomoul et al. JACC 2006
Mid-wall enhancement: Morbidity and Mortality A. Mortality or hospitalization for CV cause B. Adjusted for age, LV/RV EF, LV volumes, digoxin • VT • VT Adjusted for LVEF Assomoul et al. JACC 2006
DE confers increased risk • 65 patients with non-ischemic dilated CMP, EF < 35%, underwent CMR at baseline, followed for 17 months • 42% showed LGE at baseline • Non-ischemic pattern • 44% of those with LGE had adverse event vs. 8% without (HF, ICD discharge, death) Wu, JACC 2008
DE and risk in non-ischemic CMP Wu, JACC 2008
Functional Recovery with Medical Treatment • 45 patients with CHF treated with beta-blocker, CMR with DE at baseline and 6 month follow-up • 62% ischemic (of those 100% with DE) • 38% non-ischemic (of those only 2% with DE) • Transmurality of DE predicted contractile improvement, change in EDV and ESV Bello et al. Circ 2003
Functional Recovery with Medical Treatment Bello et al. Circ 2003
Prediction of CRT outcome by CMR • 23 patients who qualified for CRT underwent CMR at baseline, follow-up at 3 months for wall motion, 6 min walk, QOL • 50% history of MI • 57% demonstrated response • DE amount lower in responders • <15% of LV mass – 85% sens., 90% spec. • Septal transmurality of < 40% - 100% sens/spec. White et al. JACC 2006
Prediction of CRT outcome by CMR White et al. JACC 2006
Conclusions for dilated CMR • Absence of any DE is good (non-ischemic) • Predicts likelihood of recovery • Better outcomes with CRT • Lower likelihood of events
Case Example • Symptomatic improvement with ARB, beta blocker • Referred for CRT
Case Example 58 year old woman with class II-III HF symptoms referred for echo
Case Example HF with preserved LV function, grade II-III diastolic dysfunction
Differential Diagnosis • Etiology in this case is more important • Hypertensive remodeling • Hypertrophic Cardiomyopathy • Infiltrative Cardiomyopathy • Amyloidosis • Storage disease (Anderson Fabry) • Heavy metal deposition (hemochromatosis)
Utility of CMR • Not necessary to define LV volumes, although mass quantification useful • DE CMR • Etiology • Prognosis
Does LVH from HTN have DE? • 83 patients with LVH from AS (25%), HTN (31%), and HCM (44%) underwent CMR • DE seen in all etiologies • AS 62%, HTN 50%, HCM 72% • Only distinctive pattern from HCM • Generally associated with increased mass Rudolph, JACC 2009
CMR in LVH Rudolph, JACC 2009
CMR in Amyloidosis • Abnormally long myocardial T1 after Gd • Normal ≈ 1100 ms, amyloid ≈ 1400 ms • Rapid clearance of gadolinium from blood pool, abnormal distribution kinetics • Render blood pool dark • Challenging to obtain optimal myocardial nulling • Global, sub-endocardial pattern described Maceira et al. Circ 2005, Krombach, JMRI 2007
CMR in Amyloidosis Maceira: Circulation 2005
CMR in Amyloidosis • Normal protocol • 0.1 to 0.2 mmol/kg wait 15-20 mins • Modified amyloid protocol • 0.1 mmol/kg wait 5 mins Diffuse DE, poor myocardial nulling
Diffuse DE seen in Cardiac Amyloidosis Van den Driesen et al. AJR 2006
Performance of CMR in Amyloid • Sensitivity 80%, specificity 94%, PPV 92%, NPV 85% Vogelsberg et al, JACC 2008
CMR predictors of events • Amount or presence of DE does not predict mortality • Amount of DE relative to LV mass does correspond to heart failure symptoms Ruberg et al, AJC 2009
CMR in Cardiac Amyloidosis Amyloidosis with cardiac involvement Amyloidosis without cardiac involvement Ruberg et al,AJC 2009
CMR in Cardiac Amyloidosis Ruberg et al,AJC 2009
CMR in Cardiac Amyloidosis • Intramyocardial T1 gradient between epi- and endo-cardium predictive of survival • DE/LGE was not Maceira et al, JCMR 2009
CMR in Anderson Fabry • 32 Fabry patients treated with a-glactosidase, CMR obtained at baseline, followed for 3 years • 63% had fibrosis by DE, 27% did not • Absence of fibrosis associated with improved function, reduced mass, improved exercise capacity Weidemann et al., Circ 2009
CMR in Anderson Fabry Weidemann et al., Circ 2009
CMR in hemochromatosis • T2* weighted imaging • T2* abnormally shortened in iron deposition • Widely explored for thalassemia With chelation treatment (deferoxamine/deferiprone), T2* increases correlate to functional improvement in LVEF Tanner et al. Circ 2007
Case example • Diagnosis: Amyloidosis • LGE present but can tell patient not predictive of poor outcomes • Underwent stem cell transplant in 2005, doing well today, HF symptoms are controlled
Conclusions • In dilated CMP, absence of DE portends: • Recovery of LV function with medical treatment • Lower likelihood of death or hospitalization for HF • Higher likelihood of response to CRT • In dilated CMP, presence of DE • Identification of ischemic etiology and provides information in respect to revascularization recovery • Increased risk of adverse event and lower CRT response
Conclusions • In CMP with LVH/wall thickening, CMR with DE imaging can: • Identify etiology of CMP • Follow response to treatment • Associate with clinical outcomes • CMR with DE is useful as baseline exam in all forms of cardiomyopathy