Download
1 / 52
530 likes | 544 Views
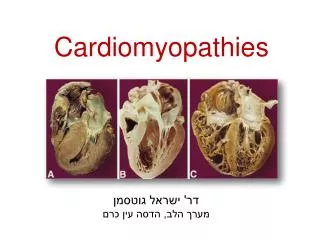
The Cardiomyopathies. Raphael Rosso M.D. group of disorders in which the dominant feature is direct involvement of the heart muscle not the result of pericardial, hypertensive, congenital, or valvular diseases

E N D
The Cardiomyopathies Raphael Rosso M.D
group of disorders in which the dominant feature is direct involvement of the heart muscle • not the result of pericardial, hypertensive, congenital, or valvular diseases • ischemic cardiomyopathy is an imprecise term to describe the condition in which CAD causes multiple infarctions, diffuse fibrosis, or severe ischemia that leads to left ventricular dilation with congestive heart failure
Dilated cardiomyopathy • Hypertrophic cardiomyopathy • Restrictive cardiomyopathy • Arrhythmogenic right ventricular cardiomyopathy • Unclassified cardiomyopathy diseases that do not fit readily into any category. Examples include systolic dysfunction with minimal dilation, mitochondrial disease, and fibroelastosis.
Dilated Cardiomyopathy • cardiac enlargement and impaired systolic function of one or both ventricles • incidence reported is 5-8 cases/ 100,000/year • three times more frequently in blacks and males as in whites and females • fourth of the cases of congestive heart failure in the United States are due to DCM
50% is idiopathic: -genetic theory25% genetic mutation, autosomal dominant transmission, mutations in genes that encode cytoskeletal, nuclear membrane, or contractile proteins, including desmin, titin, and troponin T -viral myocarditis 15% of patients with DCM have biopsy evidence of myocarditis, high antibody viral titers, viral-specific RNA sequences, and apparent viral particles in patients with "idiopathic" DCM. PCR confirmed the presence of viral remnants in the myocardium of some patients with cardiomyopathy
-autoimmunity association with HLA-DR4, antimyocardial antibodies, clinical improvement in the manifestations of heart failure in some but not all patients treated with immunoadsorption and elimination of anti-beta1-adrenergic receptor antibodies ( conversely, a randomized trial of immune globulin in recent-onset DCM showed no benefit) , influence of TNF-alpha • non-idiopathic DCM -alcohol (1/3 of DCM) -cocaine abuse -HIV -metabolic abnormalities -cardiotoxicity of anticancer drugs (especially doxorubicin)
Clinical Manifestations • middle age, more frequently men • symptoms usually develop gradually • symptomatic patients the course is usually one of progressive, annual mortality for patients with heart failure is between 11%-13% • relatively small number of patients develop symptoms of heart failure for the first time after recovery from what appears to be a systemic viral infection • a minority of patients can improve suddenly
Symptoms the most striking symptoms of DCM are those of left ventricular failure, fatigue and weakness, pulmonary congestion,systemic or pulmonary emboli, right sided heart failure is a late manifestation associated with poor prognosis Physical examinationModerate to severe cardiomegaly; S3, S4,atrioventricular valve regurgitation, especially mitral Chest Roentgenogram Moderate to marked cardiac enlargement, especially left ventricular,pulmonary venous hypertension
ECG sinus tachycardia, atrial and ventricular arrhythmias, ST segment and T wave abnormalitiesIVCD, low amplitude • Echocardiogram left ventricular dilation and dysfunction, valve insufficency • Cardiac Catheterization left ventricular enlargement and dysfunction, mitral and/or tricuspid regurgitationelevated left- and often right-sided filling pressuresdiminished cardiac output
Prognostic features: • Low EF and increased dilatation • (S3) gallop • ventricular arrhythmias • advanced age and advanced NYHA class • failure of inotropic stimulation • right sided heart failure • reduced maximal systemic oxygen uptake (especially when below 10 to 12 ml/kg/min)
To identify potentially reversible causes of DCM, several basic screening biochemical tests are indicated: • hypophosphatemia • hypocalcemia • creatinine and uremia • hypothyroidism and hyperthyroidism • hemochromatosis • HIV • elevated troponin T levels are predictive of a worse clinical course than normal levels
Therapy: • therapy of heart failure • CRT • mitral valve repair and LVAD • cardiac transplantation
Hypertrophic Cardiomyopathy • inappropriate myocardial hypertrophy that occurs in the absence of an obvious cause for the hypertrophy (e.g., aortic stenosis or systemic hypertension) • predominantly involving the interventricular septum of a nondilated left ventricle
25% of the patients show a dynamic pressure gradient in the subaortic area that divided the left ventricle into a high-pressure apical region and a lower pressure subaortic region
The LVOT obstruction is the result of the systolic anterior motion of often elongated mitral valve leaflets against the hypertrophied septum S.A.M
the overall prevalence of HCM is low: about 0.2 percent (1 in 500) of the general population and 0.5 percent of unselected patients referred for an echocardiographic examination • familial HCM occurs as an autosomal dominant disease • the sporadic forms of the disease are due to spontaneous mutations • more than 150 different mutations have been discovered of the genes which encode cardiac sarcomere proteins
the most characteristic pathophysiological abnormality in HCM is diastolic dysfunction • HCM is characterized by abnormal stiffness of the left ventricle with resultant impaired ventricular relaxation and filling • this abnormality in relaxation produces increased left ventricular end-diastolic pressure with resulting pulmonary congestion and dyspnea
Clinical findings • the majority of patients with HCM are asymptomatic or only mildly symptomatic • the most common symptom is dyspnea, occurring in up to 90 percent of symptomatic patients • angina pectoris (found in about three-fourths of symptomatic patients), fatigue, presyncope, and syncope are also common
SCD can be the initial manifestation of HCM • most frequent in adolescents and young adults less than 30 to 35 years old • most commonly during mild exertion or sedentary activities (or during sleep), not infrequently triggered by vigorous physical exertion.
the annual incidence of SCD ranges between 2% to 4% among patients seen at tertiary referral centers and approximately 1 % in the general population • the incidence is highest (up to 6%) when HCM is diagnosed in childhood, a setting in which a family history of SCD is more likely
HCM is the most common cause of SCD in young people, including competitive athletes
Physical Examination mild cardiomegaly, apical systolic thrill and heave, brisk carotid upstroke, S4 common, systolic murmur that increases with Valsalva maneuver • Chest Roentgenogram mild to moderate cardiac enlargement, left atrial enlargement • Electrocardiogram LVH, ST segment and T wave abnormalities, abnormal Q wavesatrial and ventricular arrhythmias
Echocardiogram asymmetrical septal hypertrophy (ASH) , narrow left ventricular outflow tract, systolic anterior motion (SAM) of the mitral valve, small or normal-sized left ventricle • Cardiac Catheterization diminished left ventricular compliance, mitral regurgitationvigorous systolic function, dynamic left ventricular outflow gradient
Therapy • beta adrenoceptor blocker • calcium channel blockers • Disopyramide • Amiodarone
DDD PACING • ALCOHOL SEPTAL ABLATION • SURGERY
ICD -previous SCD (class 1 indication) -sustained VT (class 2b indication) -2 or more others major risk factors (class 2b indication) • family history • syncope • NSVT • LVH 30mm • abnormal response • to exercise ACC/AHA/ NASPE 2002 guidelines
Restrictive CMP • RCM is the least common form in Western countries • abnormal diastolic function the ventricular walls are excessively rigid and impede ventricular filling • systolic function is often unimpaired, even in many cases with extensive infiltration of the myocardium DD with constrictive CMP
A variety of specific pathological processes may result in RCM, although the cause often remains unknown • Noninfiltrative causes: -idiopathic cardiomyopathy -familial cardiomyopathy -hypertrophic CMP -Scleroderma -Pseudoxanthoma elasticum -diabetic cardiomyopathy
Infiltrative causes: -Amyloidosis -Sarcoidosis -Gaucher -Hurler disease -fatty infiltration • Storage Disease -Hemochromatosis -Fabry -Glycogen storage disease
Endomyocardial -endomyocardial fibrosis -hypereosinophilic syndrome -carcinoid heart disease -metastatic cancers -radiation -toxic effects of anthracycline -drugs causing fibrous endocarditis (serotonin, methysergide, ergotamine, mercurial agents, busulfan)
HEMODYNAMICS • The clinical and hemodynamic features of restrictive heart disease simulate those of chronic constrictive pericarditis • The characteristic hemodynamic feature in both conditions is a deep and rapid early decline in ventricular pressure at the onset of diastole, with a rapid rise to a plateau in early diastole dip and plateau
Square root sign W or M pattern of RAP
square root sign • M or W waveform in the atrial pressure tracing • a wave is prominent and often of the same amplitude as the v wave • systemic and pulmonary venous pressures are elevated
Differential diagnosis with constrictive CMP • hemodynamic features • restrictive heart disease typically have left ventricular filling pressures that exceed right ventricular filling pressure by more than 5 mm Hg; this difference is accentuated by exercise, fluid challenge,and Valsalva maneuver • plateau of the right ventricular diastolic pressure is usually at least one-third of the peak right ventricular systolic pressure in patients with constrictive pericarditis, whereas it is frequently lower in RCM
endomyocardial biopsy • CT • radionuclide angiography • MRI • surgery
Symptoms Dyspnea, fatigue,Right-sided congestive heart failure, signs and symptoms of systemic disease, e.g., amyloidosis, iron storage disease • Physical Examination Mild to moderate cardiomegaly; S3 or S4, atrioventricular valve regurgitation; inspiratory increase in venous pressure (Kussmaul sign) • Chest Roentgenogram mild cardiac enlargement, pulmonary venous hypertension
ECG Low voltage, IVCD, atrioventricular conduction defects • Echocardiogram Increased left ventricular wall thickness and mass, small or normal-sized left ventricular cavity, normal systolic function, pericardial effusion • Cardiac Catheterization Diminished left ventricular compliance,"Square root sign" in ventricular pressure recordings,preserved systolic function, elevated left- and right-sided filling pressures
Therapy • The prognosis in RCM is variable; if symptomatic progression and high mortality • no specific therapy (other than symptomatic) is available for the idiopathic form of RCM, but several of the secondary forms may benefit from targeted treatment regimens (e.g., the cardiomyopathy related to iron overload, which is improved by removal of the iron, and Fabry disease, in which enzyme replacement therapy has demonstrated efficacy).
ARVD • myocardial cell loss due to apoptosis with partial or total replacement of right ventricular muscle by adipose and fibrous tissue
ARVC is associated with reentrant ventricular tachyarrhythmias of right ventricular origin often precipitated by an exercise-induced discharge of catecholamines and are a harbinger of sudden death • one-third of the cases there is autosomal dominant inheritance of the disease • ryanodine receptor (hRYR2) mutations
the diagnosis of AVRC is based on a constellation of clinical, ECG, histological, and echocardiographic findings • typical features include the appearance of clinical manifestations in adolescence or early adulthood, male predominance, normal physical examination, inverted T waves in the right precordial ECG leads, symptoms of palpitations and syncope, and a risk of sudden death