Download
1 / 27
290 likes | 464 Views
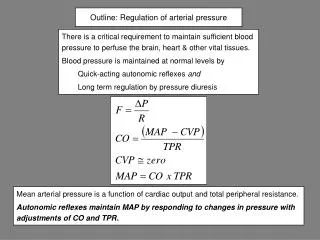
Regulation of Flow and Pressure. A. Arterial Pressure (overview) 1. Arterial pressure pulse 2. Mean arterial pressure MAP = mean arterial pressure, P s = systolic pressure, P d = diastolic pressure.

E N D
A. Arterial Pressure (overview) • 1. Arterial pressure pulse • 2. Mean arterial pressure • MAP = mean arterial pressure, • Ps = systolic pressure, Pd = diastolic pressure For regulation, you only get to change two things: the cardiac output (heart rate, stroke volume) and the resistance of the vasculature
B.-Regulation of Flow: • -Arteriolar walls have a very high ratio of smooth vascular muscle can change resistance on command. “ resistance vessels”. • -Most of the resistance to flow occurs at the arteriolar level. • Review of VSM contraction:
1. Intrinsic regulation: Local control • a. Autoregulation of arterioles (in the absence of external stimuli) • i. Myogenic mechanism : response to mechanical stimulus (or autocrine). • -VSM relaxes when the pressure in the vessel is reduced and contracts when it increases . i.e.- b) • -Net effect: maintenance of near constant blood flow for a particular metabolic level.
ii. Endothelial responses • a) Endothelium also releases vasodilator (NO) in response to blood flow • b) Ionic (Ca++ or Na++) change lead to vasoconstriction or dilation. • c) Also Endothelial Relaxation Factor.
b. Metabolic regulation : • Metabolic activity produces vasodilators as a “waste” product increased diameter lower resistance greater flow: • “Active hyperemia” (increased BF as a result of increased metabolic activity) • i. constrictors: O2 (weak) • ii. dilators: C02, H+, K+ (from muscle contractions), adenosine, NO, prostaglandins, Pi (phosphates) • iii. Lowered pH because of CO2 • CO2 + H2O HCO3- + H+ • iv. Smooth muscle has a Basal tone (just like skeletal muscle, except that it’s not independent of neuronal activity)
c. Blood Pressure Regulation: “reactive hyperemia”. • If you cutoff blood flow temporarily, and then re-open it, • the vessels will try to restore the BP constant even if it means excess Blood Flow. (this is common in strokes) • How? • “back-propagation” of vasodilatation all the way to the arteries : • i. accumulation of vasodilator metabolites is enough to reach back • ii. increased arteriolar flow increased shear stress endothelium relase of EDRF.
1. 3. Extrinsic Mechanisms • a. • A).Central nervous system connections descend from medulla in brain. In addition to sensors, cognitive/emotional response from hypothalamus and cerebrum • i. Sympathetic connections • 1. “pressor” center in medulla: (sympathetic / stimulatory: vasoconstriction, increases in heart rate, myocardiac contractility) . • 2. Tonically active (see above) and modulated by hormones and local blood pressures. • 3. transmitter used is Norepinephine (vasoconstrictor) • 4. Systemic – ie- modulated by hormones. • 5. Most effective in venous system.
ii) Parasympathetic connections • 1. “depressor”(parasympathetic / inhibitory) areas of medulla. • 2. Acetylcholine as vasodilator. • 3. Selected organs: bradykinin (vasoldilator). Produced by salivary ,and sweat glands upon parasympathetic stimulation.
iii. Differentiation between “capacitance” and “ resistance” vessels: • capacitance vessels are more passive, less sensitive to neuronal inputs because they lack beta-adrenergic receptors ( less basal tone). More common in muscles. Capacitance vessels can still react to physiological conditions (ie- they will contract in response to hypotension). • Resistance vessels are more common in the skin and actively shunt blood toward where it’s needed,
B. Blood Pressure Regulation - • b. Arterial Baroreceptors: (provide input to medulla) • i. Inhibit the sympathetic neural connections • ii. Respond directly to chances in arterial BP (and indirectly blood volume, cardiac output, TPR) • iii. Short term regulation • a) Venous BP increases better atrial filling cardiac output • b) Arteriole constriction total peripheral resistance increases
Regulation of Blood Pressure: arterial an venous control in the short term, blood volume in the long term. • Arterial Baroreceptor responses : Stretch receptors • Location: • -Carotid sinuses and aortic arch (main ones, responsible for short term changes) , • -heart (atria)) : vagal response. Can divert flow to/from kidneys through glomerular constriction, and just increase in Blood Pressure. • -lungs: also vagal response. Inspiration can reduce BP slightly
b. Hormonal • i.Adrenal glands • a) Norepinephine, epinephrine: alpha-adrenergic effect: low concentration vasodilation, beta-adrenergic effect: high concentrations vasoconstriction. • ii. Kidneys: Angiotensin II (vasoconstrictor) - Renal hypertension • c. Indirect factors • i. E.g. Adenosine Endothelium NO Vasodilation • d. Chemical mediators • i. Some agents change the sensitivity of VSM to Ca++
f. chemoreceptors: same Aortic/carotid sinuses receptors that regulate respiratory rate have some effect on the vasoconstriction of VSM, via the medulla. (when competing with the baroreceptors, though, they lose). • Hypercapnia , hypoxia , low pH all cause peripheral vasoconstriction. • Locations: Cerebellum, hypothalamus, sking and viscera. Pulmonary reflex, central chemoreceptors • Chemoreceptors in medulla produce strongest response. …
Note competition between intrinsic and extrinsic regulation of blood flow. The more vital/intolerant to hypoxia an organ is, the more intrinsic control it gets over its blood flow (brain/heart…) Dominant Intrinsic control: brain, heart, ACTIVE skeletal muscle Dominant Extrinsic control: skin, digestive, RESTING skeletal muscle
4. Venous and cardiac Effects: The system as a big circuit A. Veins are very compliant, not very resistive, but there is still a venomotor tone. Cerebral ischemia triggers venous constriction to bring up mean blood pressure. B. Unidirectional valves C. Large Blood Volume (60% of total) D. Venous Volume at the Vena Cava determines how much blood will be available for the next stroke volume, but that volume is a function of the stroke volume. Because of the “wiring”, the cardiac output drives the venous volume.
R Ca Cv Pretty Good approximation in the real world, but CAREFUL: venous volume has an effect on the cardiac output too! The heart will not pump any more blood out than what it receives. (consider what happens with bleeding, edema, dehydration ... )
Vascular function curves: vary cardiac output artificially, what happens to venous pressure. reflects lag between cardiac output and venous pressure right after diastole Note the difference in compliance between arteries and veins:
Arteriolar responses: constriction, dilation … Think of them in terms of changing resistance in the circuitry.
5. Cardiac/vascular coupling: • a. More output from the heart will rise the pressure through the system. • b. cardiac function curves: vary venous pressure artificially, what happens to cardiac output • i. Equilibrium point is where the system normally operates, can’t tolerate more than just small transient changes. • ii. Note the trajectory along the curve when you introduce a change. • iii. e.g: Sympathetic stimulation greater cardiac contractilityshift cardiac function up….then settle to new equilibrium point. • iv. e.g.: Bleeding shift vascular function to the left …then settle to new equilibrium • v. e.g: change the resistancechange the slopes of the curves
d.Cardiac output = heart rate x stroke volume BUT, stroke volume is a function of heart rate too, via myocardial contractility. Non-linear relationship!
5. Long-term regulation of BP, BV i. Renal function (though vagal response to cardiovascular BP) ii. Fluid intake iii. Other factors related to fluid retention. Bleeding, vomiting, hormones, sweating …