Download
1 / 34
350 likes | 630 Views
Betsi Cadwaladr University Health Board - Patient Safety Goals for BCUHB. Tuesday 11 May 2010. Presenter: Dr Brian Tehan, AMD – Patient Safety. Betsi Cadwaladr University Health Board. Ysbyty Glan Clwyd. Ynys Môn. Flintshire. Ysbyty Gwynedd. Conwy. Ysbyty Maelor. Denbighshire. Wrexham.

E N D
Betsi Cadwaladr University Health Board - Patient Safety Goals for BCUHB Tuesday 11 May 2010 Betsi Cadwaladr University Health Board Presenter: Dr Brian Tehan, AMD – Patient Safety
Betsi Cadwaladr University Health Board Ysbyty Glan Clwyd Ynys Môn Flintshire Ysbyty Gwynedd Conwy Ysbyty Maelor Denbighshire Wrexham Gwynedd Betsi Cadwaladr University Health Board
Aim To reduce the Betsi Cadwaladr University Health Board Global Trigger Tool adverse event rate and to also reduce the mortality rate. Betsi Cadwaladr University Health Board
Outcome Primary Drivers Secondary Drivers InterventionsPlanned & proposed Leadership and a culture of safety P1. 1000 Lives implementation and spread Normalization through CPGs & workstreams Consolidate and spread The “New”- Stroke, Hospital acquired thrombosis, and Pressure Ulcers R&D process P2. Target the top causes of Death in BCU Develop the measures and use clinical data “Amenable Mortality”? The evidence base for what is efficacious Make care safer for patients As evidenced by reductions in RAMI and Adverse Event Rate The methodology for Improvement - Spread Collaborate- National Campaigns, SPN ,etc. P3. to identify and prioritise the causes of harm “Amenable Harm”? Notes Reviews, Global Trigger Tool, IR1, Complaints & Litigation, Serious Incident Reviews, External Notification BCU Governance, Stakeholder Groups etc. Involve patients and families in safety improvement P4. Validate and standardise the data Clinical engagement- challenge through use Dash-Boards for Safety
Top Priorities Rapid response to the deteriorating patient Safe provision of acute medical care CG50 NICE Infection prevention & Control Hospital Acquired thrombosis Outcome measure Compliance Betsi Cadwaladr University Health Board
The Model for Improvement What are we trying to Accomplish? How will we know that a change is an improvement? What change can we make that will result in improvement? Act Plan Study Do When you combine these 3 questions with the… PDSA cycle, you get… …the Model for Improvement Betsi Cadwaladr University Health Board
1000 Lives Plus and Intelligent Targets Existing interventions that will continue as mini-collaboratives: • Preventing stroke through timely management of Transient Ischaemic Attack (TIA) • Rehabilitation following Stroke • Reducing Chronic Heart Failure • Transforming care – including Reducing Hospital Acquired Pressure Ulcers and falls in hospital • Preventing Hospital Acquired Thrombosis • Rapid Response to Acute Illness (RRAILLS) • Improving Medicines Management • Reducing Healthcare Associated Infections Betsi Cadwaladr University Health Board
1000 Lives Plus and Intelligent Targets New mini-collaboratives to be introduced from May 2010 onwards: • Depression • Dementia • Preventing Acute Coronary Syndrome • Patient Identifiers • Enhanced Recovery after Surgery • Reducing Falls in Intermediate Care • Maternity Services Betsi Cadwaladr University Health Board
Reducing avoidable harm and mortality WHO / NPSA Surgical Checklist SBAR Communications Trigger Tools Leadership Patient Stories Model for Improvement Normothermia Critical Care Bundles Acute Stroke 1000 Lives Plus and Intelligent Targets Improvement methodologies and maintenance of interventions – through Web-Ex and teleconferencing: Betsi Cadwaladr University Health Board
Adverse event rate Data collection commenced SPI1 2004 – Glan Clwyd Hospital SPI2 2006 – Wrexham Maelor Hospital GTT 2008 - NWW Betsi Cadwaladr University Health Board
BCUHB CHKS Diagnosis Codes Betsi Cadwaladr University Health Board
Leadership • Patient Safety Steering Group set up • Making patient safety a priority at high level meetings –dashboard developed • Patient stories polices agreed for use across BCUHB – agreed programme of use of Patient Stories • Previously established Executive WalkRoundsTM – process and programme for BCUHB under development Betsi Cadwaladr University Health Board
Executive WalkRoundsTM Betsi Cadwaladr University Health Board
Global Trigger Tool Alignment of processes across BCUHB • Inclusion and exclusion criteria • Number of reviewers • To apply to notes of patients discharged from April 2010 Betsi Cadwaladr University Health Board
Primary Care Trigger Tool “The Annual Operating Framework includes the use of the Primary Care Trigger Tool in one in twenty practices. Currently, there are no practices in North Wales consistently using this tool. Consideration needs to be given on how BCU HB encourage and support this work in GP Practices.” 1000 Lives BCUHB organisational briefing, April 2010 For further information please contact:- Andrea.hobbs@wales.nhs.uk Betsi Cadwaladr University Health Board
Communication Do you have a good news/success story to share? A template for sharing your story across BCUHB and possibly in the local media is available from Sylvia.hughes@wales.nhs.uk Please help to Spread the learningand celebrate the successes Betsi Cadwaladr University Health Board
Leadership “Executive leadership plays a key role in identifying and driving spread of reliable processes – it is therefore imperative for the organisation to identify executive leads for all content areas. Tier 1 and tier 2 posts are now well established and all should be participating in Leadership Walk Rounds.” 1000 LivesOrganisational Briefing, April 2010 Betsi Cadwaladr University Health Board
Leadership Betsi Cadwaladr University Health Board
Critical Care “Central Venous Catheter (CVC) and Ventilator Care (VC) bundles are well established and sustained across the three sites; the sepsis bundles (sepsis six, sepsis resuscitation and sepsis management) continue to need further improvement focus to produce the same level of reliability. Communication across the three sites is very good – with sharing of good practice and improvement facilitated by the network.” 1000 Lives BCUHB organisational briefing, April 2010 Betsi Cadwaladr University Health Board
Critical Care Betsi Cadwaladr University Health Board
Rapid Response to Acute Illness “The campaign team are aware from attendance at the learning sets that the BCU HB teams are involved in this content area but there is paucity of reliable process data on the extranet to comment on progress. There was excellent work on investigating the cardiac arrest data (east) after a signal within the data identified an increased rate. It is important that any findings from the investigative case note reviews that result in the planning of improvement work is implemented using the methodology advocated by the campaign – the Model for Improvement.” 1000 Lives BCUHB organisational briefing, April 2010 Betsi Cadwaladr University Health Board
Rapid Response to Acute Illness Betsi Cadwaladr University Health Board
Medicines Management “Localised work ongoing but very little pace associated with the improvement of warfarin management processes, especially across the interface between primary and secondary care – process mapping event held before the end of 2009 does not appeared to have progressed.” 1000 Lives BCUHB organisational briefing, April 2010 Betsi Cadwaladr University Health Board
Healthcare Associated Infections “Hand hygiene in secondary care, alongside antibiotic stewardship in both primary and secondary care, remain the key process measures in relation to driving down the incidence of Clostridium Difficile and MRSA. Hand hygiene compliance is not sustained above 95% across the organisation (for medical, surgical and critical care areas) although critical care has demonstrated an improvement in the east – but this is against a background of reduced observation sample size. Antibiotic stewardship demonstrates reliability in both primary and secondary care areas but again this appears to be illustrated in test/pilot areas only.” 1000 Lives BCUHB organisational briefing, April 2010 Betsi Cadwaladr University Health Board
Healthcare Associated Infections Betsi Cadwaladr University Health Board
Hospital Acquired Pressure Ulcers Betsi Cadwaladr University Health Board
Surgical Complications “Well established, reliable process measures are sustained for this work stream across all acute sites. Initial engagement with community care (i.e. the use of the WHO checklist and appropriate hair removal) has commenced to support the roll out of these interventions.” 1000 Lives BCUHB organisational briefing, April 2010 Betsi Cadwaladr University Health Board
Surgical Complications Betsi Cadwaladr University Health Board
Hospital Acquired Thrombosis “There is very little engagement with this mini-collaborative at present. The only measurement submitted to support the process of risk assessment, appropriate prescribing and administration of thrombo-prophylaxis currently includes only elective surgical patients, and not medical patients; therefore it is recommended that the leadership team at BCU HB nominate a lead to support participation in this content area.” 1000 Lives BCUHB organisational briefing, April 2010 Betsi Cadwaladr University Health Board
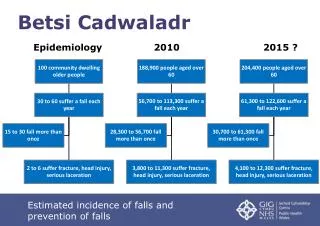
Intelligent Targets – how much by when Betsi Cadwaladr University Health Board
Organisational Briefing Key Recommendations The Campaign would endorse the following to ‘stack the cards’ in the favour of Health Boards achieving their goals and aspirations. • Take a strategic approach to quality improvement: Building the will to make measurable systemic improvement as quickly as possible. This will needs to be generated at all levels, and needs to include the will of senior leaders to make new ways of working more attractive and engage staff commitment and enthusiasm. Encouraging and spreading ideas about alternatives to the status quo which are robust enough to form the basis of new working systems; and also ideas about how to introduce them. Attending relentlessly to the execution of an aligned range of improvement initiatives into the daily work of the organisation. Betsi Cadwaladr University Health Board
Organisational Briefing Key Recommendations • Ensure a data-driven approach to measuring progress is maintained in the Health Board. Have the ability to understand the variation in your system and turn data into intelligent and useful information. Boards need to recognise that organisation level measures can mask variation between services. The capability to drill down to examine service level mortality and harm is therefore essential. • Reliable processes are the key to shifting outcomes. It is essential for leaders to set expectations and use process improvement measures to hold teams to account for local progress. • Identify executive leads for each work stream and , working with each content team, devise spread plans to enable the good work tested within the pilot areas to be rolled out in a structured and coordinated manner. 1000 Lives BCUHB organisational briefing, April 2010 Betsi Cadwaladr University Health Board
Organisation Briefing Overview “BCU HB has demonstrated throughout the life of the campaign its ability to take on new interventions and successfully test and implement changes through the use of PDSA’s and supported by continuous measurement. What is evident, via the extranet progress reporting is that the ability to spread outside the pilot areas has proved challenging and this limits the effect that process reliability will have on organisational outcomes. Spread is not organic and can only be affected by the continued structured application of the methodology and strong executive and clinical leadership.” 1000 Lives BCUHB organisational briefing, April 2010 Betsi Cadwaladr University Health Board
Organisation Briefing Overview “Participation and commitment of individuals and teams from BCU HB have been highly visible in the majority of work streams. The campaign team have identified that there are significant ‘enablers’ across the organisation, but as their capacity is often limited to their own area of expertise, their ability to drive spread is restricted. Increased capability and capacity must be a priority for BCU HB, if the existing campaign interventions are to be reliably sustained and spread and new interventions are to be taken on and successfully tested and implemented by the organisation.” 1000 Lives BCUHB organisational briefing, April 2010 Betsi Cadwaladr University Health Board