Download
1 / 6
60 likes | 66 Views
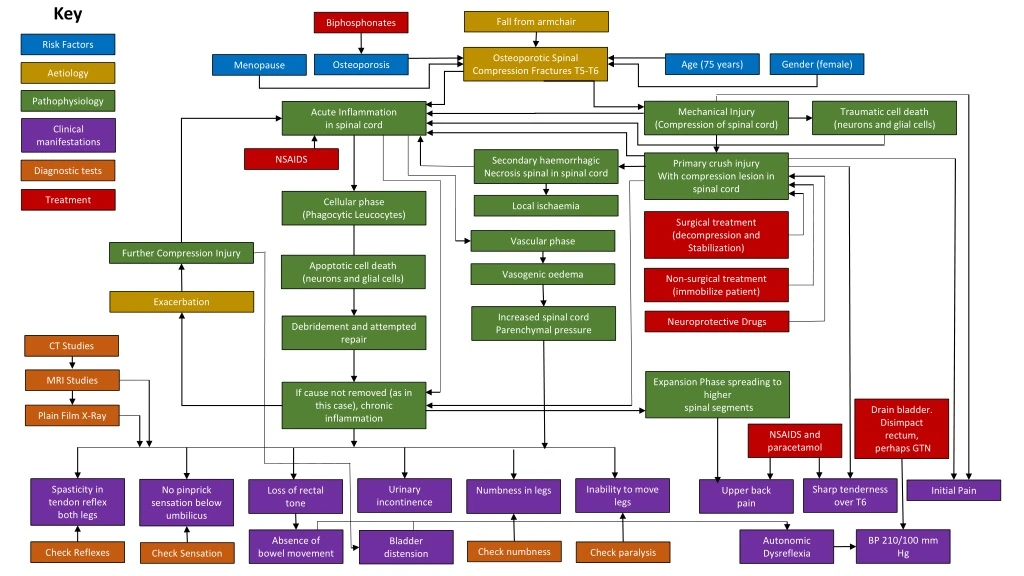
This case study explores the risk factors, pathophysiology, clinical manifestations, and diagnostic tests for traumatic spinal cord injury in a female patient with osteoporotic spinal compression fractures. It discusses the initial mechanical injury, subsequent expansion phase, and resulting neurologic deficits. The role of inflammation, apoptosis, and neuroglial activation in exacerbating the injury is also examined. The importance of early diagnosis and appropriate treatment is highlighted.

E N D
Key Fall from armchair Biphosphonates Risk Factors Osteoporotic Spinal Compression Fractures T5-T6 Age (75 years) Gender (female) Osteoporosis Menopause Aetiology Pathophysiology Traumatic cell death (neurons and glial cells) Mechanical Injury (Compression of spinal cord) Acute Inflammation in spinal cord Clinical manifestations NSAIDS Secondary haemorrhagic Necrosis spinal in spinal cord Primary crush injury With compression lesion in spinal cord Diagnostic tests Treatment Cellular phase (Phagocytic Leucocytes) Local ischaemia Surgical treatment (decompression and Stabilization) Vascular phase Further Compression Injury Apoptotic cell death (neurons and glial cells) Vasogenic oedema Non-surgical treatment (immobilize patient) Exacerbation Increased spinal cord Parenchymal pressure Neuroprotective Drugs Debridement and attempted repair CT Studies MRI Studies Expansion Phase spreading to higher spinal segments If cause not removed (as in this case), chronic inflammation Drain bladder. Disimpact rectum, perhaps GTN Plain Film X-Ray NSAIDS and paracetamol Spasticity in tendon reflex both legs Urinary incontinence Inability to move legs Sharp tenderness over T6 No pinprick sensation below umbilicus Upper back pain Loss of rectal tone Numbness in legs Initial Pain BP 210/100 mm Hg Absence of bowel movement Autonomic Dysreflexia Bladder distension Check numbness Check Reflexes Check paralysis Check Sensation
Falls are the second most common cause of traumatic spinal cord injury (TSCI) worldwide (Kumar, Lim, Mekary, Rattani, Dewan, Sharif, & Park, 2018; Zhou, Sansur, Xu, & Jia, 2017). Wilma’s risk factors include her age (75) and skeletal fragility due to her osteoporosis (Schousboe, 2016), and any previously undiagnosed condition that may have predisposed her to fall. The aetiology was her fall, causing (or exacerbating previously unrecognized) T5-T6 vertebral fractures. Since osteoporosis greatly increases the likelihood of subsequent vertebral fractures (Broy, 2016), it is possible that subsequent fractures beginning around two weeks ago led to the worsening of her condition, and an overnight shift in vertebral bone, or disk herniation, may have caused spinal cord compression with the acute symptoms and signs she now displays.TSCI is a two stage process involving initial mechanical injury causing inflammation and apoptosis, followed by a further expansion phase involving destruction of neurons and glia extending damage to higher spinal segments (Zhang, Yin, Xu, Wu, & Chen, 2012). Resulting neurologic deficits are commonly expressed by the ASIA Impairment Scale (American Spinal Injury Association 2000; Shuld, Franz, Brüggemann, Heutehaus, Weidner, Kirshblum, & Ruppon, 2016). Wilma’s initial pain was likely due to T5-T6 vertebral fracture and local inflammation, with minimal initial spinal compression. However, compression of her spinal cord has been increasing over the last two weeks resulting in urinary incontinence and loss of rectal tone. Last night, a significant primary crush injury occurred, possibly from vertebral or disk subluxation, disrupting axons and the blood-spinal cord barrier (Zhou et al., 2017). Cellular damage triggered inflammation, including haemorrhage and ischaemia with an influx of immune leucocytes and free radical-induced cell death of neurons and glial cells compounding the local injury (Zhang et al., 2012). Demyelination of neurons and activation of remaining neuroglia released further pro-inflammatory mediators (Zhou et al., 2017). These initial changes resulted in altered sensory and motor function (Zhou et al., 2017). Damage to fasciculus gracilis (sensory) and the lateral corticospinal and rubrospinal tracts (motor) among others resulted in the distribution of her numbness, absence of skin-prick sensation, and leg paralysis (Engelhardt & Sobotzik, 2017). Dorsal spinal compression also interrupts the sensory pathway from the bladder (Engelhardt & Sobotzik, 2017), meaning the micturition centre in the pons (Barrington’s nucleus) is not receiving appropriate stimulation to empty the bladder. There is a
descending spinal component in relation to defaecation (Frenckner, 1975), compromising which may result in loss of rectal muscle tone and constipation. Her hypertension may reflect autonomic dysreflexia, possibly from unrecognized bladder distension (Partida, Mironets, Hou, & Tom, 2016). The expansion phase will spread the damage to higher spinal segments, increasing the extent of the injury within the first week (Zhang et al., 2012).Wilma’s medical history and clinical assessment, including the recognition that the presentation is bilateral, will inform the diagnosis. Common differentials include neoplasia, osteomyelitis leading to epidural abscess, and epidural haematoma (Ropper A.E., & Ropper, A.H., 2017), and others include hyperparathyroidism and other metabolic conditions underlying clinical osteoporosis (Cicala, Briganti, Casale, Rossi, Cagini, Cesarano, Brunese, & Giganti, 2013). Diagnostic tests include initial CT because it is sensitive to detection of fractures and subluxation, followed by MRI to demonstrate any disk herniation, oedema and haemorrhage, or ligament damage (Ropper A.E., & Ropper, A.H., 2017). MRI is useful in distinguishing between metastatic neoplastic lesions and acute osteoporotic compression fractures (Cicali et al., 2013). Dynamic and/or standing plain-film radiographs may also be useful in addition (Joaquim, Patel, Schroeder, & Vaccaro, 2018). Initial medication may include analgaesia before movement and transport, and for immediate control of blood pressure. Middleton, Ramakrishnan, & Cameron (2014) discuss treatment of autonomic hyperreflexia. Longer term control of blood pressure is aimed at optimizing spinal perfusion. Nonsteroidal anti-inflammatory drugs, calcitonin, teriparatide, and bisphosphonates may be given (Genev, Tobin, Zaidi, Khan, Amirouche, & Mehta, 2017). Medications including methylprednisolone sodium succinate, minocycline and naloxone may be neuroprotective (Santamaria & Guest, 2017). Long-term cellular therapies are also being investigated (Leung, 2012). Wilma may need to be immobilized during evaluation (Reid, 2018). Injuries with borderline stability such as this may require subsequent surgical decompression and stabilization (Joaquim et al., 2018) including percutaneous fixation procedures such as screws, kyphoplasty (Caruso, Lombardi, Andreotti, Lorousso, Gildone, Padovani, & Massari, 2018) or vertebroplasty (Zhang, Liu, Wu, Xie, Qin, & Huang, 2018). These approaches have the potential to reduce pain, and may improve the quality of life (Genev et al., 2017), although they are not without risks of recollapse (Li, Guo, Zhang, Liang, Yuan, Mo, Li, Guo, Tang, & Luo, 2018).
References • American Spinal Injury Association. (2000). International Standards for Neurological Classifications of Spinal Cord Injury (pp. 1-23). • Broy, S. B. (2016). The Vertebral Fracture Cascade: Etiology and Clinical Implications. Journal of Clinical Densitometry, 19(1), 29-34. 10.1016/j.jocd.2015.08.007. • Caruso, G., Lombardi, E., Andreotti, M., Lorousso, V., Gildone, A., Padovani, S. & Massari, L. (2018). Minimally Invasive Fixation Techniques for Thoracolumbar Fractures: Comparison between Percutaneous Pedicle Screw with Intermediate Screw (PPSIS) and Percutaneous Pedicle Screw with Kyphoplasty (PPSK). European Journal of Orthopaedic Surgery & Traumatology. doi: 10.1007/s00590-018-2122-1 • Cicala, D., Briganti, F., Casale, L., Rossi, C., Cagini, L., Cesarano, E., . . . Giganti, M. (2013). Atraumatic Vertebral Compression Fractures: Differential Diagnosis between Benign Osteoporotic and Malignant Fractures by MRI. Musculoskeletal Surgery, 97(S2), 169-179. 10.1007/s12306-013-0277-9 • Engelhardt, M. & Sobotzik, J-M. (2017). Functional Neuroanatomy of the Spinal Cord. In Weidner, N, Rupp, R. & Tansey, K. E. (Eds.), Neurological Aspects of Spinal Cord Injury (Chapter 2). Springer, Switzerland. https://doi-org.libraryproxy.griffith.edu.au/10.1007/978-3-319-46293-6 • Frenckner, B. (1975). Function of the Anal Sphincters in Spinal Man. Gut, 16(8), 638-644. 10.1136/gut.16.8.638. • Genev, I. K., Tobin, M. K., Zaidi, S. P., Khan, S. R., Amirouche, F. M. L., & Mehta, A. I. (2017). Spinal Compression Fracture Management: A Review of Current Treatment Strategies and Possible Future Avenues. Los Angeles, CA: SAGE Publications.10.1055/s-0036-1583288 • Joaquim, A. F., Patel, A. A., Schroeder, G. D. & Vaccaro, A. R. (2018). A Simplified Treatment Algorithm for Treating Thoracic and Lumbar Spine Trauma, The Journal of Spinal Cord Medicine.doi: 10.1080/10790268.2018.1433267
Kumar, R., Lim, J., Mekary, R., Rattani, A., Dewan, M., Sharif, E. O., & Park, K. B. (2018). Traumatic Spinal Injury: Global Epidemiology and Worldwide Volume. World Neurosurgery. https://doi.org/10.1016/j.wneu.2018.02.033 • Leung, L. (2012) Cellular Therapies for Treating Pain Associated with Spinal Cord Injury. Journal of Translational Medicine, 10 (37). https://doi.org/10.1186/1479-5876-10-37 • Li, Y. X, Guo, D.Q., Zhang, S.C., Liang, Yuan, K., Mo, G.Y., Li,. D.X., Guo, H.Z., Tang, Y. & Luo, P.J. (2018). Risk Factor Analysis for Re-Collapse of Cemented Vertebrae after PercutaneousVertebroplasty(PVP) or PercutaneousKyphoplasty(PKP). International Orthopaedics. doi: 10.1007/s00264-018-3838-6 • Middleton, J., Ramakrishnan, K. & Cameron, I. Treatment of Autonomic Dysreflexia for Adults and Adolescents with Spinal Cord Injuries. Agency for Clinical Innovation. (2014). Retrieved from https://www.aci.health.nsw.gov.au/__data/assets/pdf_file/0007/155149/Autonomic-Dysreflexia-Treatment.pdf • Partida, E., Mironets, E., Hou, S., & Tom, V. J. (2016). Cardiovascular Dysfunction Following Spinal Cord Injury. Neural Regeneration Research, 11(2), 189-194. doi: 10.4103/1673-5374.177707. • Reid, D. B. C. (2018). Spinal Cord Compression. In Ferri, F.F. (Eds), Ferri’s Clinical Advisor (pp. 1197-1199). Retrieved from http://hy8fy9jj4b.search.serialssolutions.com.libraryproxy.griffith.edu.au/?ctx_ver=Z39.88-2004&ctx_enc=info%3Aofi%2Fenc%3AUTF-8&rfr_id=info%3Asid%2Fsummon.serialssolutions.com &rft_val_fmt=info%3Aofi%2Ffmt%3Akev%3Amtx%3Abook&rft.genre=book&rft.title=Ferri%27s+clinical+advisor+2018&rft.au=Ferri%2C+Fred+F&rft.series=Ferri%27s+medical+solutions&rft.date=2017-05-25&rft.pub=Elsevier&rft.isbn=9780323280495&rft.externalDocID=9780323529570¶mdict=en-AU
Ropper, A., & Ropper, A. (2017). Acute Spinal Cord Compression. New England Journal of Medicine, 376(14), 1358-1369. 10.1056/NEJMra1516539 • Santamaria, A.J. & Guest, J.D. (2017). The Current Status of Neuroprotection for Spinal Cord Injury. In Weidner, N, Rupp, R. & Tansey, K. E. (Eds.), Neurological Aspects of Spinal Cord Injury (Chapter 20). Springer, Switzerland. Retrieved from https://doi-org.libraryproxy.griffith.edu.au/10.1007/978-3-319-46293-6 • Schuld, C., Franz, S., Bruggemann, K., Heutehaus, L., Weidner, N., Kirshblum, S., . . . EMSCI study group. (2016). International Standards for Neurological Classification of Spinal Cord Injury: Impact of the Revised Worksheet (revision 02/13) on Classification Performance. Journal of Spinal Cord Medicine, 39(5), 504-512. 10.1080/10790268.2016.1180831 • Schousboe, J. T. (2016). Epidemiology of Vertebral Fractures. Journal of Clinical Densitometry, 19(1), 8-22. 10.1016/j.jocd.2015.08.004 • Zhang, N., Yin, Y., Xu, S., Wu, Y., & Chen, W. (2012). Inflammation & Apoptosis in Spinal Cord injury. Indian Journal of Medical Research, 135(3), 287-296. • Zhou, K., Sansur, C., Xu, H., & Jia, X. (2017). The Temporal Pattern, Flux, and Function of Autophagy in Spinal Cord Injury. International Journal of Molecular Sciences, 18(2), 466. 10.3390/ijms18020466 • Zhang, Z.E., Liu, D.H., Wu, P.Y., Xie, C.L., Qin, F.W. & Huang, H. (2018). Ultra-Early Injection of Low-Viscosity Cement in Vertebroplasty Procedure for Treating Osteoporotic Vertebral Compression Fractures: A Retrospective Cohort Study. International Journal of Surgery, 52, 35-39. 10.1016/j.ijsu.2018.02.025