Download
1 / 30
340 likes | 497 Views
Overview of Maternal in South Sudan. Ministry of Health Republic of South Sudan presented by Dr Alexander Dimiti , DG RH MOH RSS. 4 th December 2013, Juba Bridge Hotel Hotel Juba. Outline of Presentation. Introduction & Background Situational analysis Strategic direction

E N D
Overview of Maternal in South Sudan. Ministry of Health Republic of South Sudan presented by Dr Alexander Dimiti, DG RH MOH RSS. 4th December 2013, Juba Bridge Hotel Hotel Juba.
Outline of Presentation • Introduction & Background • Situational analysis • Strategic direction • Implementation modalities • Costs and Financing of the HSDP • Conclusion
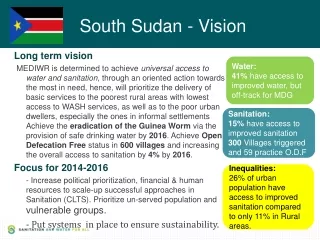
Introduction & Background • Government of the Republic of South Sudan is committed to reduction of Maternal and Child mortality • South Sudan Development Plan(SSDP) 2011-2013 prioritizes reduction of Maternal & child mortality • Health Sector Development Plan 2012 to 2016 • Goal and objectives of the HSDP further emphasizes improvement in maternal and child health
Introduction & Background cont’d • Current MNH related policies & strategies • National Reproductive Health Policy and Strategy • Family Planning Policy • Basic Package of Health & Nutrition Services • Country Multiyear Plan for Expanded Program on Immunization • MNH Action Plan is informed by these documents as well as the HSDP • Development of a Comprehensive MNH strategy
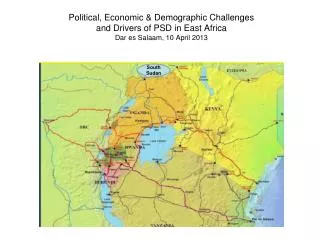
Situational Analysis cont’d • Political Context • 5 decades of liberation war[1955-2005] disrupted all infrastructure & social services including health systems • Close 2.5 million deaths & 4 million displaced • INGOs & FBO assumed responsibility for health service provision in liberated areas • CPA signed in 2005 till July 2011 when RSS attained independence, assuming full responsibility for service delivery • Administrative organization • 10 states; 80 counties; 514 payams
Situational Analysis contd,d • Demographic & Socio-economic status • Population estimated; 8.3 million • Sparse population density 15 people/Sq KM • 90% population live in rural areas • Growth rate: 3% • Total Fertility Rate: 7.1 • Life expectancy[both sexes]: 57 years • Popn living on less than 1US$ a day: 51% • Access to portable water: less than 50% • Access to proper sanitation: less than 7% • Illiteracy rates: women:88%; men:63%
South Sudan National Assessment for Emergency Obstetric & Newborn Care October 2013 UN Guidelines recommend at least 5 EmONC facilities (including at least one comprehensive facility) for every 500,000 people. Applying these standards to South Sudan’s 2012 projected population of 10,864,357, It is estimated that South Sudan should have 109 EmONC facilities: 87 Basic EmONCfscilities & 22 Comprehensive EmONC facilities.
South Sudan National Assessment for Emergency Obstetric & Newborn Care October 2013 cont’d: According to the assessment South Sudan has 24:14 comprehensive EmONC facilities, & 10 Basic EmONC facilities, Therefore there is a deficit of 77 Basic EmONC and 8 Comprehensive EmONC facilities. Analysis of the data by facility type revealed that of all 50 hospitals, 13 (26%) were Comprehensive, 3 were Basic (6%) & 19 (38% were partial, & 15 (30%) did not perform the minimum number of signal functions (Non-EmONC complaint).
South Sudan National Assessment for Emergency Obstetric & Newborn Care October 2013 cont’d: Of the 181 PHCCs 1 (0.5%) was Comprehensive, 7 (4%) were Basic , 44 (24%) were partial, & 129 (71%) were non-EmONC.
Key findings EmOC NA– HMIS & Charts Poor quality of charts reviewed 1.Partographs not routinely used for decision making 2.HMIS poor 3.Documentation of obstetric complications 4.Maternal deaths 5. Stillbirths and neonatal death 6. Referral
Key findings EmOC NA – Equipment, drugs & supplies Government & partners are most important source of drugs for all sectors Causes of delays in delivery of supplies Administrative problems Transportation difficulties
Cause of death • Leading direct causes: • Haemorrhage – 34% • Hypertension – 19% • Unsafe abortion – 9% • Sepsis – 9% • Understanding the cause of death distribution is important for program development and monitoring
Priority Inventions for Scale up • Maternal Health priority interventions • Scale up focused Antenatal Care • Skilled attendance at birth • Scale up Emergency Obstetric & Newborn Care • Institutionalize postnatal care • Scale up family planning • Expand PMTCT services • Prevention and prompt treatment of Malaria • Immunization for Tetanus
Priority actions for acceleration cont’d Reposition of RH in MOH structure RH directorate created among the 9 Develop a comprehensive MNCH strategy Based on the gaps identified during the EmONC NA, EmONC Investment Plan process has started to be completed in January 2014.
Priority actions for acceleration cont’d • Human Resources Capacity for effective delivery of MNCH service • Strengthening midwifery & nursing education Plans to increase the No of NHTIs to 6 & increase the No of Nursing & Midwives students by Jan 2014. • Train specialists (Obstetricians/Gynecologists; Pediatricians, neonatologists) -30 OBGYN specialists training has started with support of WHO & UNFPA. • 2 Medical Doctors at University of Nairobi (OBGYN); 2-4 Medical officers selected to Universities in Ethiopia
Updates on Task Shifting On going Scholarship Initiative: 8 students in Zambia; 20 Clinical Officers selected to go to Malawi College of Health Sciences (10 integrated EmONCand Surgery; 10 Clinical Officers – anaesthesia; Training of for Clinical Officers in task-shifting locally to start in Jan 2014 in Jongolei.
Updates on Task Shifting cont’d Curriculum finalization discussions on setting a TWG to be set up before the end of 2013. Discussions on setting up a Policy Team tom come up policy recommendations for Task Shifting Initiative.
Priority actions for acceleration cont’d Recruit & deploy available professional midwifes/Project supported by UNFPA started in April 2013: Currently 12 professional midwives in 7 states. New professional midwives are currently being recruited 11 have so far arrived in the country All 11 have completed their orientation with the MOH Letters of introduction to the states have been provided by the Undersecretary MOH. Midwives will be based across all states of South Sudan including sites where midwifery schools are based. Skills improvement of current cadres(MCH nurses, CHW/CMW) through in-service training
Priority actions for acceleration cont’d • Infrastructural development for delivery of MNCH services • Construction/rehabilitation of 8 Maternity hospitals in 8 States including theatres, Modernization of 3 Teaching and 7 State Hospitals including completion of Warrap State Hospital, PHCC, PHCU • Secure essential equipment for delivery of MNH services: • Equipment for all hospitals, PHCC,PHCU, • Advocacy for increased allocation of government resources to the health sector, especially for MNCH
Priority actions for acceleration cont’d • Strengthen community based MNH intervention • Strengthen outreaches & skills of CHWs • Scale up provision of MNH interventions at hospitals, PHCC,PHCU • Ensure equitable availability & access across health facilities within the country • Strengthen systems for monitoring and reporting on MNCH interventions • Reviews of maternal, perinatal & neonatal deaths
Priority actions for acceleration cont’d • Strengthen health commodities security • Secure regular supply of essential medicines and supplies for MNCH • Review of nation wide RHCS situation analysis, operational plan & quantification done with support of JSI/Deliver.
EmONC NA Conclusions Near absence of BEmONC facilities Low numbers of CEmONC facilities Underperformance of 3 Signal functions Mortality due to PPH, Obstructed Labour, APH & Abortion complication Limited PMTCT services
Recommendations (1) Strengthen 44 partial BEmONC status to full BEmONC status Strengthen 19 partial CEmONC status to full CEmONC status Strengthen referral system from BEmONC to CEmONC
Recommendations (2) Inclusion of EmONC in training curricula Refresher trainings: Early newborn care BEmONC (MVA, Vacuum etc) Post abortion care
Recommendations (3) Access to blood supplies/blood banks Use of best practice guidelines Rapid expansion of PMTCT Strategy for cervical cancer screening Strengthening HMIS, LMIS & HRIS 24 Hour access to water & electricity
Recommendation 3From Data to Action Planning: Dissemination Action planning & implementation Women are the fabric of society in South Sudan. Let us not allow them to continue dying from preventable causes as they give life! This is the golden hour