Download
1 / 24
240 likes | 313 Views
18wRTT Delivery - The Pathway Re-engineering Challenge. Denis Gizzi. Measuring V Delivering. The most defined measurement system will still only quantify a business process. RTT end-to-end stage recording, tracking & reporting is priceless,

E N D
18wRTT Delivery - The Pathway Re-engineering Challenge Denis Gizzi
Measuring V Delivering The most defined measurement system will still only quantify a business process. RTT end-to-end stage recording, tracking & reporting is priceless, BUT WON’T ,ON IT’S OWN, DELIVER AN 18 WEEK TOTAL CARE PATHWAY EXPERIENCE FOR PATIENTS
Learning So Far (re stage 1)local pioneer work • Engineering is not difficult – culture change is • 18 week delivery is higher on the commissioner radar • Pragmatic & basic data collection systems are possible • Don’t assume basic systems are in place (e.g. clinic outcomes) • Easier to make changes where systems are owned • Commissioner should drive data specification • Sufficient knowledge in the system to drive through objectives • Diagnostic end-to-end stage measurement is critical • Define generic outcome collection 1st rather than consult • RTT for ICATS/T2 segment of pathway presented NO material problem • Interim IT solutions will have to suffice (until CFH delivers) • Variable understanding of 18wRTT & how fits with broader reform • Clinical engagement (or lack of) is an overused excuse for poor business planning
Learning So Far (re stage 1)Wider Pioneers • Focus on business process change (define our data) • Get ready for the commissioner challenge (is this defined?) • Technical system change is not feasible (i.e. through PAS) • Easier to make changes because we own the process & system • Very little commissioner participation in RTT measurement • Diagnostic end-to-end stage measurement is critical • Defining generic outcome collection sheets is easy, getting consultants to use it isn’t • Interim IT solutions will have to suffice (until CFH delivers) • Variable understanding of 18wRTT & fit with broader system and policy reform • Reconciling tactical RTT measures with core business systems is challenging! • Supporting reform products (e.g. ICATS) & wider alignments is vague
Commissioner led Pioneer – the specific challenges • The PCT does not own or have defined operational knowledge of hospital PAS systems. • We do not have a direct management relationship with hospital clinicians who are faced with 18wRTT changes. • Commissioning & contractual levers for change require greater definition. • Aligning reform programmes with 18wRTT requirements & keep the financial plates spinning in sequence. • Raising the profile of WIP (re 18wRTT) to the top of everyone's agenda. • Raising the bar – re Business Processes • Programme spread throughout Economy
Delivering & Sustaining 18wRTTThe Care Pathway Challenge(Stage 2)
Driving 18wRTT Pathways – The Realisation • The days of negotiating, cajoling, modernising to improve outcomes has come to an end? • Specifications & agreed systematic pathways will drive lean outcomes • Commissioning levers & incentives are critical (harvest local clinical knowledge & capacity) + expect financial penalties • Drive continuous improvement via market management • Systemising care processes, moving away from variation & disparate decision management for 80% of care processes. • Disciplined (objective based) decision management (at each–to-end stage) is critical
The challenge of 18 weeks The NHS needs to continue to reduce waits to first assessment and from decision to treat to treatment. This will require more activity and reform than ever before. In addition the NHS needs to focus on the time from first assessment to decision to treat which historically has not been a major focus. 18 Weeks GP OP D OP IP GP Visit 1st OutpatientAppointment Decision to treat Treatment The time from the first (assessment) outpatient to decision to treat includes the most significant challenges including all diagnostics and subsequent outpatients
Generic Pathway to be managed – Adapted from (DOH) model GP CAS Assessment CAS Diagnostics CAS Referral 1st OP Diagnostics 2nd OP DTA On booked list 1st IP Treatment in OP CAS Treatment • Commissioners need to drive delivery across this entire pathway • Re-define the key stages along the pathway that PCTs need to monitor • Standard thresholds & accountabilities at each stage to reduce variation • ICATS / CASs (or equivalent) must be lean & deliver VFM & BR • So what sort of business intelligence systems are required to enable this?
Knowledge System Challenge for Pathways The 3 essential components High Level - Strategic Real Time - Operational (WIP) Consumer Facing Enabling High-Level Performance Reporting Enabling Dynamic / Real Time WIP Review Enabling the Informed Service User 100% planned, ordered, timed & structured 18wRTT journey By Provider & Specialty (inc ICATS, IS Diag) By Provider & Specialty (inc ICATS, IS Diag) By HRG / Procedure Pathway (inc ICATS, CAS) Aligned & Integrated BIS Solutions CAB-CAS-OP-Diag-Therapies-Surgery-Financial & Output Reporting CPA & Optimisation Reports Unique tagging & tracking – Know the Work in Progress (WIP) at any point in time The focus for continuous improvement
Care Pathway Management (CPM) – Objectives Defining the High-Level Objectives • Remove variability in consumer experience • All consumers have a structured and ordered care experience • Accountabilities are described for each step within the pathway • Resources are available at each step of the pathway • Fixed standards (performance & outcomes & metrics) are clearly described • 18w pathways are policy compatible & deliver value for money • All 18w service providers work to a common set of standards • Consumers and clinicians as equal partners in pathway design
Care Pathway Management (CPM) – Outputs Defining the Core Outputs • All consumers complete their RTT experience within 18weeks • All consumers feel empowered and informed • All CPM navigators (e.g. GPs) feel empowered and informed • Zero consumer complaints concerning RTT experience • Financial aspects of 18wRTT Care Pathways are described, structured, agreed and reportable. • Performance of 18wRTT Care pathways is measurable and reportable. • Standards for 18wRTT Care Pathways are stated, agreed, costed & reported
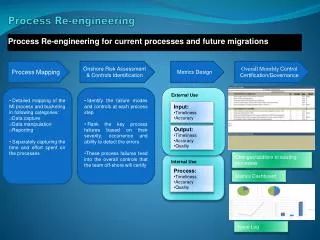
Our Approach in OldhamCommissioner Led - Lean Pathway Engineering 8 Stage Process • RTT Measurement Systems (define the Work in Progress) • Systematically analyse all (18wRTT) pathways & inefficiencies • Engineer-out the sub optimal / non value adding aspects • Re-define the optimal pathway (cement the lean process) • Specify the optimal pathway as the (commissioners) product requirement • Procure the product to the specified quality & capacity standards (via the market & commercial processes) • Performance manage (know the WIP & expected outcomes)and assure delivery • Continuous improvement (re-engineer the variations)
Our Approach in OldhamCommissioner Led - Lean Pathway Engineering The Plan • Assess baseline current RTT performance for top 13 specialties • Select top 25 high volume symptom / procedure pathways • Undertake research on well-grounded pathway for each • Undertake clinical consultation regarding efficiencies • Overlay generic 18wRTT commissioning standard • Describe standards to provider market (inc plural pathways) • Undertake real capacity planning to ensure financial & PH probity • Gauge views from clinical “firms” regarding their views on opportunities • Cement pathway maps into local prospectus & contracting regimes
Risks & Challenges RTT tactical measurement solutions (for all 18w pathways) are required now. Work within clinical partnerships to re-engineer systems now. No slack time in the system (strategic IT solution won’t deliver in time) Assurance systems – embryonic at best (trust professional knowledge) RTT & data systems – specified for each pathway deliverer Next Steps DSCN compliant processes Real demand & capacity planning 18wRTT systematic pathway reviews Capacity & Specialty engineering Specifications & Commissioning Performance & tracking & Incentives Clinical ownership of pathway maps Disciplined thinking, planning & operational execution (J.Coultard HSJ 29/06/06) Commissioning Pathways Summary
18wRTT & PTL A Commissioners Approach
PTL & the Commissioner • Has to add value • Has to be deliverable (with little or no added investment) • Has to be accurate & timely • Can not be merely Old School WL systems • Has to be core product within business cycle • Applies to all segments in the supply chain • Is critical to market management, therefore has to be a dynamic & timely product with correct design features
Waiting list, queue = what we should have done Demand = All requests for a service = what we should do Capacity = what we could do Activity = what we did Traditional Elective System Waiting list is a tool used to store WIP until a ‘do something critical’ point’ is reached. PTLs are fixed points in systems (OP & IPE) – Risk of breach is mitigated by supply chain data capture Not enough attention, therefore ill defined, variable & unregulated Core business planning for service operators – should commissioners describe it for them? PTLs convert to activities – but little commissioner input & insufficient assurance
Scheduled & Organised Assessment Control = Available Diagnostics & Measured Outputs (RTT) + Alignments to physical (community) resources Demand = All requests Meet defined standards & are UBRN controlled Capacity = defined turnaround requirement Activity = what we planned to undertake Care Pathway Management Approach Waiting list is obsolete Scheduling & segmentation & tracking is the key PTL Control is critical!! How are we assured? The commissioner should determine & direct “what should be done” via specifications & commercial rigour Real Capacity Plans & tracking & assurance process (PTLs) For PCT & PBC Partners to define, reduce variability. PBC to determine regulatory (governance) framework Core business planning for service operators – commissioners should define a slot based procurement model This should align with commissioner specification & assurance processes (PTLs)
18wRTT – Pathway & PTL Non Admitted PTL These stages will require significant culture change GP CAS Assessment CAS Diagnostics CAS definitive decision Consent & Pre-op Booked theatre slot TCI Action Discharge & Charge Total End-End Stage has defined parameters Admitted Pathway PTL Via CAB & UBRN generated CAS Treatment Total End-to-End Stage has defined parameters RED = Do something significant points
PTL Principles – For Commissioners The Basics • Rules for assessment control have to be set • Rules for differentiating Admitted V Non Admitted • Rules for Clinical outcome (decision recording) • No patient added to list without booked TCI slot • Trigger “assurance” points defined for each • Standard Data collection items defined • Patients enter APP after DSCP is reached (not before) • Core business processing “cemented” in SLAs • Shared customer & supply chain knowledge system
Driving Faster Reform via Standardised (transferable) Processes Generic 18wRTT Pathway Commissioning Template Via Clinical Partnership agreements Including internally generated demand (con-to-con) (led by PBC) • Decision Threshold • Define minimum referral management standards • Define minimum work-up (the diagnostic pack) • UBRN based ordering • Slot based capacity matching Capacity maps for each delivery component & stage RTT CLOCK STARTS • Assessment Control • Agreed set of pathways • Defined set of diagnostic capacity • Objective based decision management • Lean process management & UBRN based ordering • Time defined outputs • Integrated pathway management (direct listing) • Contractual performance metrics, incentives & penalties Re-engineered services and/or re-procured Outpatient as ICATS (outputs within 4 weeks average 6 weeks maximum) + RTT recording & PTL tracking Provider Choice & Dynamic Market Management Consistent standards for all providers (outputs within 9 week average 14 week maximum) + RTT recording & PTL tracking • Decision to Treat & Action • Define minimum direct listing standards • Define minimum work-up (1st & 2nd line diagnostic pack) • UBRN based ordering • Slot based capacity matching • Contractual performance metrics, incentives & penalties
PTL sounds OK – the catch! • PCTs can’t own PTL production • PTLs act as assurance / mitigation / tactical tools • Supply chain owns WIP & therefore PTLs • Model contracting for PTL production & access • DSS = do something significant = triggers • Currently no reference spine for UBRN across path • PCT charged with assurance & customer navigation • PTLs need careful specification & production • What would PCTs do with them & how often?