Download
1 / 26
350 likes | 746 Views
Malaria Endemic Areas and Drug Resistance. Chloroquine resistance. SP resistance. Multi-drug resistance. Plasmodium life cycle. Introduction. Chloroquine had became the treatment of choice since its discovery in 1930 due to the following facts: Cheap Safe

E N D
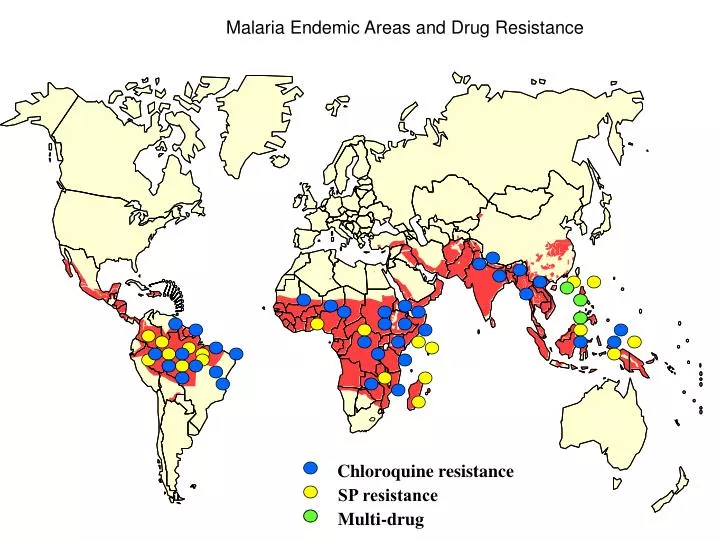
Malaria Endemic Areas and Drug Resistance Chloroquine resistance SP resistance Multi-drug resistance
Introduction • Chloroquine had became the treatment of choice since its discovery in 1930 due to the following facts: • Cheap • Safe • Initially highly effective drug • it was the cornerstone of the effort to eradicate malaria in the 1950s and 1960s
Chloroquine resistance • CQ-resistant Plasmodium falciparum arose and was first detected in Southeast Asia and South America in the late 1950s (Peters, 1969), • Reaching Africa two decades later (Campbell et al., 1979; Fogh et al., 1979, 1984; Jepsen et al., 1983).
Chloroquine resistance • Within 10 years, CQ resistance began to reach high levels in many parts of Southern and Eastern Africa. • In response to unacceptably high rates of CQ failure, in 1993 Malawi became the first sub-Saharan African country to discontinue the use of CQ and shift to sulfadoxine–pyrimethamine nationwide (Bloland et al., 1993). • Subsequently, Kenya, Botswana and Tanzania also adopted the policy change from chloroquine to sulfadoxine–pyrimethamine nd other combination
Drug resistance- definition: It is the “ability of a parasite strain to survive and/or multiply despite the administration and absorption of a drug given in doses equal to or higher than those usually recommended but within tolerance of the subject”.
Degree of resistance: assessment WHO has developed a simple scheme for estimating the degree of the resistance that involves studying the parasitemia over 28 days. Smears on day 2 , 7 and 28 are done to grade the resistance as RI to RIII.
Sensitive (S): The asexual parasite count reduces to 25% of the pre-treatment level in 48 hours after starting the treatment and complete clearance after 7 days, without subsequent recrudescence - Complete Recovery. RI, Delayed Recrudescence: The asexual parasitemia reduces to < 25% of pre-treatment level in 48 hours, but reappears between 2-4 weeks. RI, Early Recrudescence: The asexual parasitemia reduces to < 25% of pre-treatment level in 48 hours, but reappears earlier. RII Resistance: Marked reduction in asexual parasitemia (decrease >25% but <75%) in 48 hours, without complete clearance in 7 days. RIII Resistance: Minimal reduction in asexual parasitemia, (decrease <25%) or an increase in parasitemia after 48 hours.
WHO modified in vivo test • Minimum follow up 14 days Early treatment failure (ETF): Development of danger signs or severe malaria on Day 1,2,3 in the presence of parasitaemia Late clinical failure (LCF) Development of danger signs or severe malaria after day 3 in the presence of parasitaemia Late parasitological failure (LPF): Presence of parasitaemia on any day from day 7 to day 28 and temp below 37.5 oC Adequate clinical and parasitological response (CPR): Absence of parasitaemia on day 28 irrespective of auxiliary temp
Molecular basis of CQ resistance • CQ is thought to exert its antimalarial effect by interfering with hematin detoxification in the digestive vacuole of the parasite. • PfCRT is a predicted transporter located on the digestive vacuole membrane and may be responsible for modulating CQ accumulation within vacuole. • Mutation of PfCRT is strongly associated with in vitro resistant isolates
Factors associated with resistance • Longer half-life. • Genetic mutation. • Poor compliance • Host immunity. • Number of people using these drugs. • Poor compliance.
Malaria Endemic Areas and Drug Resistance Chloroquine resistance SP resistance Multi-drug resistance
Treatment of drug-resistant malaria-new policy • This strategy is based on use of combination therapy based on artemisinin derivatives offers hope to preserving the efficacy of antimalaria drugs and prolonging their useful therapeutic. • Artemether+Sulfadoxine/pyrimethamine (1st line) • Artesunate +lumefantrine(2nd line) • Quinine (3rd line as well a the drug of choice for treatment of severe malaria)
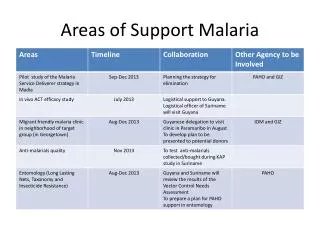
The current situation of malaria in Sudan • 80 % of the population in Sudan are living in malarial endemic areas. • In spite of presence of all type of Malaria parasite, Plasmodium falciparum causes 80-90% of infections. • Prevalence of malaria ranged between (17.4 – 44.8%) in out – patient clinics and (9.6-36.3.8%) in in-patients. • Death rate is ranging between (0.9 – 6.9%) . (Federal Ministry of Health, 2003).
Chloroquine resistance in SudanHistoric background 1 • The presence of CQ resistant parasites strains in Sudan was first suggested by Omer A. M. and Moyou, S, (1979) in Gezira area and by Kouznestov, A. A. et al.,1979) in Sennar. • This was later confirmed by an in vitro study at Gezira area (Ibrahim (1986).
Chloroquine resistance in Sudan Historic background 2 • Later was reported in Khartoum State (Al Tawil & Akood M A 1983). The report indicated that the level of resistance was up to RIII levels. • Further studies carried out by Baynoumi, R. A et al., (1989) have indicated the emergence of chloroquine resistance in eastern part of Sudan.
Chloroquine resistance in Sudanlatest results • In north and central part of Sudan the level of CQ resistance is near 50% Report on sentinel sites , National malaria administration 1999 • Out of 50 patients 12(50%) were classified as resistance in Gedaref state Babiker et al JID 2001 V 183
Important factors that are associated with resistance: • Physiological adaptation. • Single mutation for resistance. • Longer half –life. • Host immunity. • Number of people using these drugs. • Poor compliance.
Chloroquine resistance in Sudanlatest results • In South the levels of CQ resistance is regaining from 15-80% Stivanello E et al, Trop int. health Bachy C, MSF report 2003 • 75.9% CQ resistance cases reported in Gedaref area. • 32.1% CQ resistance cases reported in Hag Yousif area Tagelsir et al. acta tropical 2006 V 79
Remerging of chloroquine susceptibility • Vietname study by Jacquire etal 1983 • The use of CQ was deceased in Vietnam since 1975. • Out of 68 patients included in the study the rate cure was 90% • The good clinical response was attributed to the decreased use of CQ since 1975.
Remerging of chloroquine susceptibility • Other studies conducted later had conflicting out comes and this attributed to the fact that the removal of CQ in Vietnam was incomplete due to its continued use for treatment of P.vivax which is absence or present in low percentage in sub-Saharan Africa
Remerging of CQ susceptibility-African experience • Malawi was the first country to switch from CQ to Fansidar for the 1st line of treatment in 1993. • 5 years after this change clinical isolates were tested in vitro for CQ susceptibility The results indicated that: • 65% of the isolates were sensitive to CQ. • 31% were border line resistance • 3% were resistant cases.
Remerging of chloroquineFuture • These studies if they confirmed by well designed controlled clinical studies, several opportunities for managing malaria drug resistance problem become possible • Reintroducing of CQ as monothreapy is highly inadvisable