Download
1 / 70
700 likes | 827 Views
Chapter 15: The Cardiovascular System. Myocardial Thickness and Function. The thickness of the myocardium of the four chambers varies according to the function of each chamber. The atria walls are thin because they deliver blood to the ventricles.

E N D
Myocardial Thickness and Function The thickness of the myocardium of the four chambers varies according to the function of each chamber. The atria walls are thin because they deliver blood to the ventricles. The ventricle walls are thicker because they pump blood greater distances The right ventricle walls are thinner than the left because they pump blood into the lungs, which are nearby and offer very little resistance to blood flow. The left ventricle walls are thicker because they pump blood through the body where the resistance to blood flow is greater.
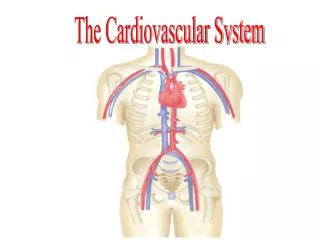
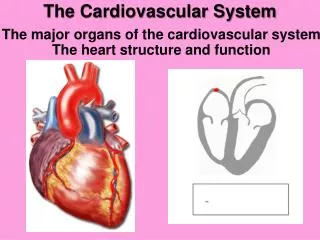
Locating the Heart Posterior to sternum medial to lungs Anterior to vertebral column Base lies beneath 2ndrib Apex at 5th intercostal space Lies upon diaphragm
Heart Chambers • Right Atrium • receives blood from • inferior vena cava • superior vena cava • coronary sinus • Right Ventricle • receives blood from right atrium • Left Atrium • receives blood from pulmonary veins • Left Ventricle • receives blood from left atrium
EXTERNAL HEART Anterior View
EXTERNAL HEART Posterior View
Right Atrium • Receives blood from 3 sources • superior vena cava, inferior vena cava and coronary sinus • Interatrial septum partitions the atria • Fossa ovalis is a remnant of the fetal foramen ovale • Tricuspid valve • Blood flows through into right ventricle • has three cusps composed of dense CT covered by endocardium
Right Ventricle • Forms most of anterior surface of heart • Papillary muscles are cone shaped trabeculaecarneae (raised bundles of cardiac muscle) • Chordae TENDINAE: cords between valve cusps and papillary muscles • Interventricular septum: partitions ventricles • Pulmonary semilunar valve: blood flows into pulmonary trunk
Left Atrium • Forms most of the base of the heart • Receives blood from lungs- 4 Pulmonary VEINS • (2 right + 2 left) Red blood in a vein? Weird! • Bicuspid valve: blood passes through into left ventricle • has two cusps • to remember names of this valve, try the pneumonic LAMB • Left Atrioventricular, Mitral, or Bicuspid valve
Left Ventricle • Forms the apex of heart • Chordae tendineae anchor bicuspid valve to PAPILLARY muscles (also has trabeculaecarneae like right ventricle) • Aortic semilunar valve: • blood passes through valve into the ascending aorta • just above valve are the openings to the coronary arteries
Atrioventricular Valves Open • A-V valves open and allow blood to flow from atria into ventricles when ventricular pressure is lower than atrial pressure • occurs when ventricles are relaxed, chordae tendineae are slack and papillary muscles are relaxed
Atrioventricular Valves Close • A-V valves close preventing backflow of blood into atria • occurs when ventricles contract, pushing valve cusps closed, chordae tendinae are pulled taut and papillary muscles contract to pull cords and prevent cusps from everting
Semilunar Valves • SL valves open with ventricular contraction • allow blood to flow into pulmonary trunk and aorta • SL valves close with ventricular relaxation • prevents blood from returning to ventricles, blood fills valve cusps, tightly closing the SL valves
Valve Function Review Atria contract, blood fills ventricles through A-V valves Ventricles contract, blood pumped into aorta and pulmonary trunk through SL valves
Fibrous Skeleton of Heart Dense CT rings surround the valves of the heart, fuse and merge with the interventricular septum Support structure for heart valves Insertion point for cardiac muscle bundles Electrical insulator between atria and ventricles prevents direct propagation of AP’s to ventricles
Heart Contraction Atrial Systole/Ventricular Diastole Atrial Diastole/Ventricular Systole https://www.youtube.com/watch?v=waOSUpEHPQs
Cardiac Cycle • Atrial Systole/Ventricular Diastole • blood flows passively into ventricles • remaining 30% of blood pushed into ventricles • A-V valves open/semilunar valves close • ventricles relaxed • ventricular pressure increases
Cardiac Cycle • Ventricular Systole/Atrial diastole • A-V valves close • chordae tendinae prevent cusps of valves from bulging too far into atria • atria relaxed • blood flows into atria • ventricular pressure increases and opens semilunar valves • blood flows into pulmonary trunk and aorta
Heart Sounds • Lubb • first heart sound • occurs during ventricular systole • A-V valves closing • Dupp • second heart sound • occurs during ventricular diastole • pulmonary and aortic semilunar valves closing Murmur – abnormal heart sound
Cardiac Muscle Fibers • Cardiac muscle fibers form a functional syncytium • group of cells that function as a unit • atrial syncytium • ventricular syncytium
Muscle Bundles of the Myocardium • Cardiac muscle fibers swirl diagonally around the heart in interlacing bundles
Electrocardiogram • recording of electrical changes that occur in the myocardium • used to assess heart’s ability to conduct impulses P wave – atrial depolarization QRS wave – ventricular depolarization T wave – ventricular repolarization
Electrocardiogram • Impulse conduction through the heart generates electrical currents that can be detected at the surface of the body. A recording of the electrical changes that accompany each cardiac cycle (heartbeat) is called an electrocardiogram (ECG or EKG). • The ECG helps to determine if the conduction pathway is abnormal, if the heart is enlarged, and if certain regions are damaged. • Figure 20.12 shows a typical ECG.
Electrocardiogram---ECG or EKG • EKG • Action potentials of all active cells can be detected and recorded • P wave • atrial depolarization • P to Q interval • conduction time from atrial to ventricular excitation • QRS complex • ventricular depolarization • T wave • ventricular repolarization
ECG • In a typical Lead II record, three clearly visible waves accompany each heartbeat It consists of:. • P wave (atrial depolarization - spread of impulse from SA node over atria) • QRS complex (ventriculardepolarization - spread of impulse through ventricles) • T wave (ventricular repolarization). • Correlation of ECG waves with atrial and ventricular systole (Figure 20.13)
ECG • As atrial fibers depolarize, the P wave appears. • After the P wave begins, the atria contract (atrial systole). Action potential slows at the AV node giving the atria time to contract. • The action potential moves rapidly through the bundle branches, Purkinje fibers, and the ventricular myocardium producing the QRS complex. • Ventricular contraction after the QRS complex and continues through the ST segment. • Repolarization of the ventricles produces the T wave. • Both atria and ventricles repolarize and the P wave appears.
Regulation of Cardiac Cycle Additional Factors that Influence HR • physical exercise • body temperature • concentration of various ions • potassium • calcium • parasympathetic impulses decrease heart action • sympathetic impulses increase heart action • cardiac center regulates autonomic impulses to the heart
CARDIAC OUTPUT • Cardiacoutput (CO) is the volume of blood ejected from the left ventricle (or the right ventricle) into the aorta (or pulmonary trunk) each minute. • Cardiac output equals the strokevolume, the volume of blood ejected by the ventricle with each contraction, multiplied by the heartrate, the number of beats per minute. • CO = SV X HR • Cardiac reserve is the ratio between the maximum cardiac output a person can achieve and the cardiac output at rest.
Cardiac Output • CO = SV x HR • at 70ml stroke volume & 75 beat/min----5 and 1/4 liters/min • entire blood supply passes through circulatory system every minute • Cardiac reserve is maximum output/output at rest • average is 4-5x while athlete’s is 7-8x
Influences on Stroke Volume • Preload (affect of stretching) • Frank-Starling Law of Heart • more muscle is stretched, greater force of contraction • more blood more force of contraction results • Contractility • autonomic nerves, hormones, Ca+2 or K+ levels • Afterload • amount of pressure created by the blood in the way • high blood pressure creates high afterload
Preload: Effect of Stretching • According to the Frank-Starling law of the heart, a greater preload (stretch) on cardiac muscle fibers just before they contract increases their force of contraction during systole. • Preload is proportional to EDV. • EDV is determined by length of ventricular diastole and venous return. • The Frank-Starling law of the heart equalizes the output of the right and left ventricles and keeps the same volume of blood flowing to both the systemic and pulmonary circulations.
Contractility • Myocardial contractility, the strength of contraction at any given preload, is affected by positive and negativeinotropicagents. • Positive inotropic agents increase contractility • Negative inotropic agents decrease contractility. • For a constant preload, the stroke volume increases when positiveinotropic agents are present and decreases when negative inotropic agents are present.
Afterload • The pressure that must be overcome before a semilunar valve can open is the afterload. • In congestive heart failure, blood begins to remain in the ventricles increasing the preload and ultimately causing an overstretching of the heart and less forceful contraction • Left ventricular failure results in pulmonary edema • Right ventricular failure results in peripheral edema.
Chemical regulation of heart rate • Heart rate affected by hormones (epinephrine, norepinephrine, thyroid hormones). • Cations (Na+, K+, Ca+2) also affect heart rate. • Other factors such as age, gender, physical fitness, and temperature also affect heart rate.
Arteries and Arterioles • Arterioles • thinner wall than artery • endothelial lining • some smooth muscle tissue • small amount of connective tissue • helps control blood flow into a capillary • Artery • thick strong wall • endothelial lining • middle layer of smooth muscle and elastic tissue • outer layer of connective tissue • carries blood under relatively high pressure
Arteriole • smallest arterioles only have a few smooth muscle fibers • capillaries lack muscle fibers
Capillaries • smallest diameter blood vessels • extensions of inner lining of arterioles • walls are endothelium only • semipermeable • sinusoids – leaky capillaries
Exchange in the Capillaries • water and other substances leave capillaries because of net outward pressure at the capillaries’ arteriolar ends • water enters capillaries’ venular ends because of a net inward pressure • substances move in and out along the length of the capillaries according to their respective concentration gradients