Download
1 / 1
10 likes | 136 Views
PHYSICIANS’ KNOWLEDGE AND ATTITUDE REGARDING THE NEW AMERICAN HEART ASSOCIATION’S GUIDELINES FOR INFECTIVE ENDOCARDITIS PROPHYLAXIS G. El-Kass, S. Heidarian, I. Dubson, R. Hussain, N. Mathew, R. Pekmezaris, Y. Dlugacz, G. P. Wolf-Klein

E N D
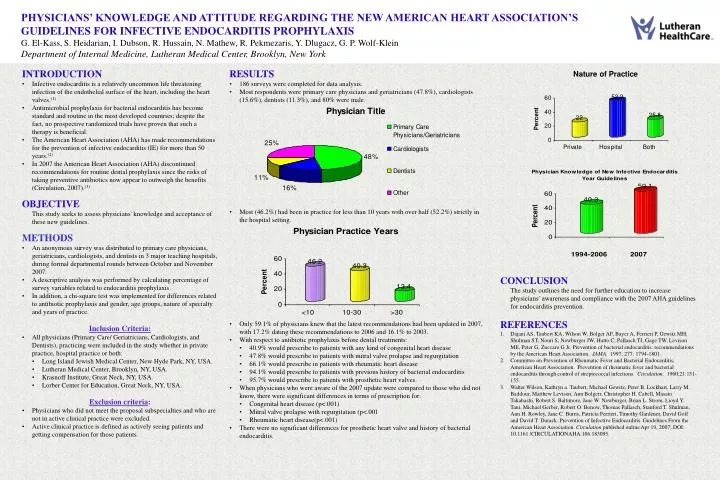
PHYSICIANS’ KNOWLEDGE AND ATTITUDE REGARDING THE NEW AMERICAN HEART ASSOCIATION’S GUIDELINES FOR INFECTIVE ENDOCARDITIS PROPHYLAXIS G. El-Kass,S. Heidarian, I. Dubson, R. Hussain, N. Mathew, R. Pekmezaris, Y. Dlugacz, G. P. Wolf-Klein Department of Internal Medicine, Lutheran Medical Center, Brooklyn, New York • INTRODUCTION • Infective endocarditis is a relatively uncommon life threatening infection of the endothelial surface of the heart, including the heart valves.(1) • Antimicrobial prophylaxis for bacterial endocarditis has become standard and routine in the most developed countries; despite the fact, no prospective randomized trials have proven that such a therapy is beneficial. • The American Heart Association (AHA) has made recommendations for the prevention of infective endocarditis (IE) for more than 50 years.(2) • In 2007 the American Heart Association (AHA) discontinued recommendations for routine dental prophylaxis since the risks of taking preventive antibiotics now appear to outweigh the benefits (Circulation, 2007).(3) • OBJECTIVE • This study seeks to assess physicians' knowledge and acceptance of these new guidelines. • METHODS • An anonymous survey was distributed to primary care physicians, geriatricians, cardiologists, and dentists in 3 major teaching hospitals, during formal departmental rounds between October and November 2007. • A descriptive analysis was performed by calculating percentage of survey variables related to endocarditis prophylaxis. • In addition, a chi-square test was implemented for differences related to antibiotic prophylaxis and gender, age groups, nature of specialty and years of practice. • Inclusion Criteria: • All physicians (Primary Care/ Geriatricians, Cardiologists, and Dentists), practicing were included in the study whether in private practice, hospital practice or both: • Long Island Jewish Medical Center, New Hyde Park, NY, USA. • Lutheran Medical Center, Brooklyn, NY, USA. • Krasnoff Institute, Great Neck, NY, USA. • Lorber Center for Education, Great Neck, NY, USA. • Exclusion criteria: • Physicians who did not meet the proposal subspecialties and who are not in active clinical practice were excluded. • Active clinical practice is defined as actively seeing patients and getting compensation for those patients. • RESULTS • 186 surveys were completed for data analysis. • Most respondents were primary care physicians and geriatricians (47.8%), cardiologists (15.6%), dentists (11.3%), and 80% were male. • Most (46.2%) had been in practice for less than 10 years with over half (52.2%) strictly in the hospital setting. • Only 59.1% of physicians knew that the latest recommendations had been updated in 2007, with 17.2% dating these recommendations to 2006 and 16.1% to 2003. • With respect to antibiotic prophylaxis before dental treatments: • 40.9% would prescribe to patients with any kind of congenital heart disease • 47.8% would prescribe to patients with mitral valve prolapse and regurgitation • 66.1% would prescribe in patients with rheumatic heart disease • 94.1% would prescribe to patients with previous history of bacterial endocarditis • 95.7% would prescribe to patients with prosthetic heart valves. • When physicians who were aware of the 2007 update were compared to those who did not know, there were significant differences in terms of prescription for: • Congenital heart disease (p<.001) • Mitral valve prolapse with regurgitation (p<.001 • Rheumatic heart disease(p<.001) • There were no significant differences for prosthetic heart valve and history of bacterial endocarditis. • CONCLUSION • The study outlines the need for further education to increase physicians’ awareness and compliance with the 2007 AHA guidelines for endocarditis prevention. • REFERENCES • Dajani AS, Taubert KA, Wilson W, Bolger AF, Bayer A, Ferrieri P, Gewitz MH, Shulman ST, Nouri S, Newburger JW, Hutto C, Pallasch TJ, Gage TW, Levison ME, Peter G, Zuccaro G Jr. Prevention of bacterial endocarditis: recommendations by the American Heart Association. JAMA. 1997; 277: 1794-1801. • Committee on Prevention of Rheumatic Fever and Bacterial Endocarditis, American Heart Association. Prevention of rheumatic fever and bacterial endocarditis through control of streptococcal infections. Circulation. 1960;21:151-155. • Walter Wilson, Kathryn a. Taubert, Michael Gewitz, Peter B. Lockhart, Larry M. Baddour, Matthew Levison, Ann Bolgerr, Christopher H. Cabell, Masato Takahashi, Robert S. Baltimore, Jane W. Newburger, Brian L. Strom, Lioyd Y. Tani, Michael Gerber, Robert O. Bonow, Thomas Pallasch, Stanford T. Shulman, Ann H. Rowley, Jane C. Burns, Patricia Ferrieri, Timothy Gardener, David Goff and David T. Durack. Prevention of Infective Endocarditis. Guidelines From the American Heart Association. Circulation published online Apr 19, 2007; DOI: 10.1161 /CIRCULATIONAHA.106.183095.