Download
1 / 55
580 likes | 1.18k Views
Cholesterol: The Expanded Lipid Profile. Ben Brown MD December 19, 2011 Thanks also to Wendy K and Fasih H. Outline. What is the expanded lipid panel? Why order it? How to order it? What to do with results? Cases Questions. Cases.

E N D
Cholesterol:The Expanded Lipid Profile Ben Brown MD December 19, 2011 Thanks also to Wendy K and Fasih H
Outline • What is the expanded lipid panel? • Why order it? • How to order it? • What to do with results? • Cases • Questions
Cases • 54 y/o woman with no risk factors and an LDL of 189. She does not want meds. • 35 y/o Latino male with new onset DM and a “perfect” lipid panel. • 40 y/o male who comes in and tells you that his Dad and brother both had their first MI at 45y/o. His lipids look more or less normal. • Bonus Case from Wendy • A 72 y/o woman obese, HTN, IGT, depression. What is my risk of heart disease or stroke?
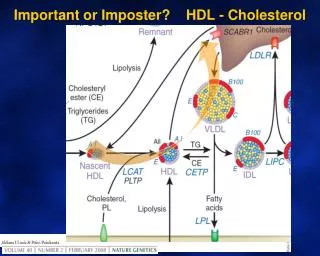
Why bother with more? • Not all lipids are the same risk: • impact of LDL size & number • HDL subtypes • In selected patients: Other Risk Factors missed with typical lipid panel • Lp(a) • hsCRP • FHx early CADz and close to normal lipids • Metabolic Syndrome and need more info to change • High Lipids and wants to avoid statins or difficulty tolerating
Question? In addition to the standard lipid profile, What is included in the expanded lipid panel? • LDL subtypes (apoB) • HDL subtypes (2 and 3) • LPa • hsCRP • Homocysteine • All of the above • It depends
Expanded Lipid Profiles • Quest: expanded lipid panel (or lipid- or homocyt- with homocysteine) • Lipoprotein Particle Analysis (LPP) Spectracell • Berkeley HeartLab (BHL) • NMR: Liposcience • VAP: Atherotec • Hunter: Cardiovascular Risk/Metabolic Syndrome
LDL: particle size and number Less is more (better) ApoB ( one per particle) scientifically accepted measurement for LDL particle number. Can be used to Monitor statintherapy. Bigger is Better • Small LDL is the bad guy why? • it goes across the endothelium more readily • absorbed by macrophages more readily = foam cells…bad
Apo B (LDL pattern) Nl <60
Case 1 According to ATP 3 Guidelines what would you recommend for our 54 y/o woman with no risk factors and an LDL of 189? • Life style with a goal of LDL 160 • Life style with a goal of LDL 130 • Start a Statin • Start Bile Acid Binder or Niacin
Case 1 According to ATP 3 Guidelines what would you recommend for our 54 y/o woman with no risk factors and an LDL of 189? • Life style with a goal of LDL 160 • Life style with a goal of LDL 130 • Start a Statin • Start Bile Acid Binder or Niacin
ATP 3 Guidelines-surprisingly generous Google: ATP 3 Guidelines at a glance
Her expanded panel results • LDL=189, TG=102, HDL =63 • apoB 20 (low) • hsCRP 0.5 (normal) • HDL2 (normal) • HDL3 (normal) • Lp(a) low • Later an AIC was 5.0 What if her Apo B or hsCRP or AIC was high?
Treatment of small dense LDL Treat LDL cholesterol and think Metabolic or Inflammation • Insulin Resistance (glycocylation) • Check AIC and treat accordingly • Note: I start metformin early in someone who does not make LS changes easily (provider choice). • Inflammation (oxidation) • Check hsCRP • Think of antioxidants • Will cover with hsCRP
HDL HDL 3 Smaller less protective (signal of inefficient transport) HDL 2 (a and b) • Again bigger is better • Reverse cholesterol transport • Antioxidant effect • Increases with exercise, fish oil, niacin, fibric acid, statin and niacin combo’s, moderate alcohol consumption.
Case 2 35 y/o Latino male with new onset DM and a “perfect” lipid panel. • TC 168 • HDL 41 • TG 115 • LDL 104 Expanded Panel • Apo B high • HDL 2 low/3 normal • Hs CRP 1.7 • Lp(a) normal What would you do?
Treatment of Low HDL 2 • Exercise • Niacin • Moderate alcohol consumption (both 2 and 3) • Stop smoking • ?Fish oil • ?statin, FibricAcids, Bile acid binder might start for high apoB • Mediterranean Diet, fish oils, consider probiotic for his high CRP
LipoProtein (a) Niacin NAC 600 mg twice daily Treatment options: • Lp(a) is an inherited abnormal protein attached to LDL. • Normal level < 30 mg/dL • Lp(a) increases coagulation and triples CVD risk.
Case 3 • 40 y/o male who comes in and tells you that his Dad and brother both had their first MI at 45y/o. His lipids look more or less normal. Expanded panel results • Lp(a) high (104) • Others normal What would you do?
Bonus case: Wendy’s patient • 58 yo woman, slender, healthy eater with h/o ischemic stroke age 58. Year later, ischemic bowel.
Inflammation Lp-PLA2 Slightly more specific for vascular inflammation Low risk <200 mg/ml Hs-CRP • Inflammatory marker • Better then ESR and leucocytes for predicting vascular events • Low Risk level < 1.0 mg/L
Treatment of increased hsCRP • Look for cause: inflammation, infection, trauma. • Consider checking Lp-PLA2 (endothelial inflammation) • Anti-inflammatory regimen • Diet (Mediterranean anti-inflammatory or mod elim) • Exercise (any is better) • Fish oils (dose by EPA/DHA 2-6g a day) • Probiotics (10 billion org a day) • Vit D (check level and treat to 50) • Decrease Stress and support good sleep (cortisol)
4th Patient • 72 y/o woman obese, HTN, IGT, depression. • “What is my risk of heart disease or stroke?” • How do you answer this question? • Very Concrete thinker • Can you do it in a way that furthers the patients motivation to change and is affordable?
Thoughts after test Routine lipid panel • At Goal • HDL = 65 • VLDL = 18 • Chol/HDL ratio =3.2 • TG’s = 90 • moderate risk • TC = 211 • LDL = 128 • Non-HDL chol = 146 Advanced Risk Markers • High Risk • hsCRP = 4.88 [<1] • sd-LDL = 36.2 [20] • Moderate Risk • Apo B 113 [<60] • Homocysteine 11.2 (<10) At Goal • Lp-PLA2 185.4 (<200)
How to treat • NCEP –ATC diet with goal of dropping 5-10% weight • Lower carbohydrate, higher fiber diet • Omega 3 fats; substitute olive oil • Screen for DM, hypothyroidism • Lower LDL*
Summary • High apoB = Small dense LDL ~ metabolic syndrome • check AIC, treat LDL earlier, LS changes, consider earlier metformin, check hsCRP • Low HDL (especially low High HDL 2) • Exercise, Niacin, moderate ETOH • High Lp(a) bad • Niacin, NAC • High hsCRP (cardio CRP) > 1.0 • r/o infection, inflammation, trauma. Repeat test/ck lp-PLA2 • Anti-inflam regimen (diet, ex, stress, fish oil, probiotic, antioxidants) • Homocysteine: a definite risk factor, interventions lower it, ?if that makes a difference unless they have the condition hyperhomocysteinuria (rare).
Homocysteine • Methylation (if high also check B12/folate/methylmalonic acid) • Functions primarily to protect DNA • How to help • For most Mediterranean Diet adequate, if still a problem may need supplementation • B6 25 micrograms/d • B12 1000micrograms/d • Folate 800micrograms/d (may need as methyl THF)
Progression of Drug Therapy in Primary Prevention If LDL goal not achieved, intensify drug therapy or refer to a lipid specialist If LDL goal not achieved, intensifyLDL-lowering therapy Monitor response and adherence to therapy Initiate LDL-lowering drug therapy 6 wks 6 wks Q 4-6 mo • If LDL goal achieved, treat other lipid risk factors • Start statin or bile acid sequestrant or nicotinic acid • Consider higher dose of statin or add a bile acid sequestrant or nicotinic acid
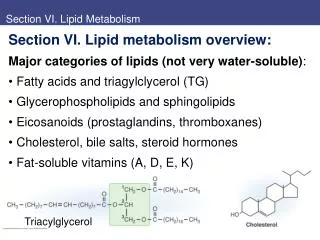
Lipids Background Cholesterol Functions • Plasma Membranes • Myelinated structures in the CNS • Inner Mitochondrial Membranes • Bile Acids • Steroid Hormones and Sex Hormones • Ergosterol(UV skin) Vit D3
Lipids Background Lipids in Atherosclerosis Dys-Function • Endothelium and damage • LDL and Macrophages • Oxidized LDL and Foam Cells • Also glycosylated and acetylated LDL • Plaque and rupture • HDL as scavenger
Cholesterol General Total Cholesterol/HDL ratio (TC/HDL) Best Lipid predictor of CHD in Framingham Study TC/HDL ratio 1 unit = CHD risk by 60% Eg TC/HDL ratio of <4 is normal 6 = 120% increased risk 3 = 60% decreased risk
Risk for coronary disease was associated with higher values of • non–HDL-C and LDL-C, • higher ratios of non–HDL-C/HDL-C • apo B/A1 (LDL/HDL) • lower values of HDL-C. • not associated with triglyceride levels • No difference in risk prediction was observed between fasting and non-fasting measurements. JAMA: 2009 68 Studies: 300,000 patients Mean fu 6 years Risk for coronary disease was associated with higher values of non–HDL-C and LDL-C, higher ratios of non–HDL-C/HDL-C apoB/A1 lower values of HDL-C. not associated with triglyceride levels No difference in risk prediction was observed between fasting and nonfasting measurements. Di Angelantonio E et al. for the Emerging Risk Factors Collaboration. Major lipids, apolipoproteins, and risk of vascular disease. JAMA 2009 Nov 11; 302:1993.
IM4U Treatment Pyramid Environment Relationships Resources
IM4U Treatment Pyramid (expanded) Environment Relationships Resources
Drug Therapy 1) HMG CoA Reductase Inhibitors (Statins) • Reduce LDL-C 18–55% & TG 7–30% • Raise HDL-C 5–15% • Major side effects • Myopathy • Increased liver enzymes • Contraindications • Absolute: liver disease • Relative: use with certain drugs
HMG CoA Reductase Inhibitors (Statins) (continued) Demonstrated Therapeutic Benefits • Reduce major coronary events • Reduce CHD mortality • Reduce coronary procedures (PTCA/CABG) • Reduce stroke • Reduce total mortality
Statins: Drug-Nutrient Side Effects Nutrients Depleted • Coenzyme Q10: Statins inhibit the enzyme HMG CoA reductase that is required to make cholesterol and Coenzyme Q10. • Could explain myalgia, exercise intolerance, myoglobuinuria • Also, Selenium, Zinc, Copper • Lower serum PUFA’s and alter the relative % of omega 6:3 fats Arch Neurol 2004;61(6):889 Nutr Metab Cardiovasc Dis 2005; 15(1): 36
Drug Therapy 2) Bile Acid Sequestrants Ex: cholestyramine, colestipol, colesevelam • Major actions • Reduce LDL-C 15–30% • Raise HDL-C 3–5% • May increase TG • Contraindications • Dysbetalipoproteinemia • Raised TG (especially >400 mg/dL)
Bile Acid Sequestrants (continued) • Demonstrated Therapeutic Benefits • Reduce major coronary events • Reduce CHD mortality • Side effects • GI distress/constipation • Decreased absorption of other drugs • Decreases beta-carotene, calcium, folate, Fe, Mg, Vit B12, D, E, K & zinc (cholestyramine)
Drug Therapy 3) Nicotinic Acid • Major actions • Lowers LDL-C 5–25% • Lowers TG 20–50% • Raises HDL-C 15–35% • Side effects: flushing, hyperglycemia, hyperuricemia, upper GI distress, hepatotoxicity • Contraindications: liver disease, severe gout, peptic ulcer
Nicotinic Acid Drug FormDose Range Immediate release 1.5–3 g(crystalline) Extended release 1–2 g Sustained release 1–2 g
Nicotinic Acid (continued) Demonstrated Therapeutic Benefits • Reduces major coronary events • Possible reduction in total mortality
Drug Therapy 4) Fibric Acids Example: gemfibrozil, fenofibrate, clofibrate • Major actions • Lower LDL-C 5–20% (with normal TG) • May raise LDL-C (with high TG) • Lower TG 20–50% • Raise HDL-C 10–20% • Contraindications: Severe renal or hepatic disease
Fibric Acids (continued) • Demonstrated Therapeutic Benefits • Reduce progression of coronary lesions • Reduce major coronary events • Side effects: dyspepsia, gallstones, myopathy • Drug-nutrient interactions: Decrease CoQ10 also, Vitamin E, (fenofibrate incr’s homocysteine)