Download
1 / 40
420 likes | 599 Views
Chylomicron Transport dietary lipids from the intestine to the peripheral tissues. VLDL – IDL - LDL. VLDL function: Deliver TG from liver to peripheral tissue cells LDL function: Deliver Cholesterol from live to peripheral tissue cells. HDL function:

E N D
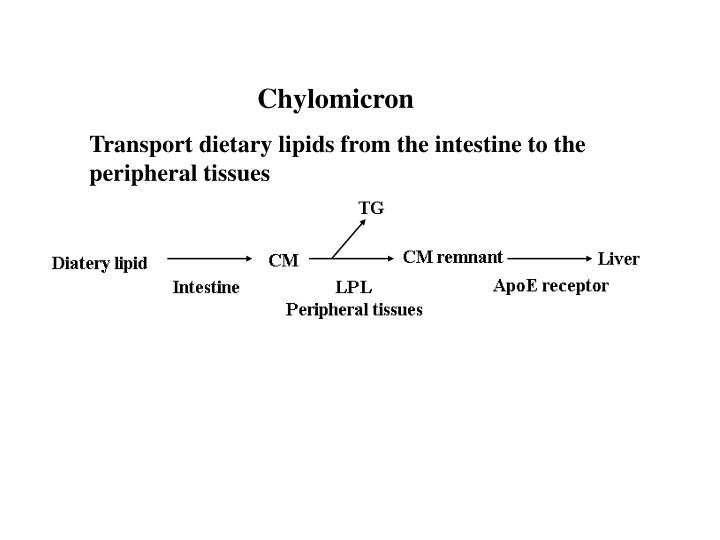
Chylomicron Transport dietary lipids from the intestine to the peripheral tissues
VLDL – IDL - LDL • VLDL function: Deliver TG from liver to peripheral tissue cells • LDL function: Deliver Cholesterol from live to peripheral tissue cells
HDL function: Reverse-transport cholesterol from peripheral cells to the liver for excretion
Cholesterol metabolism Exclusively found in animal: animal sterol 2g/kg for health person
Role of cholesterol • An essential component of cell membranes, has a vital role for membrane functions. • Used to synthesize bile acids in the liver. • Used to synthesize steroid hormones. • glucocorticoids • mineralocorticoids • androgens • estrogens • progestins • 4. Used to synthesize Vitamin D.
Cholesterol synthesis • About 1g of cholesterol is synthesized per day in adults, liver: 50%; intestine 15%; other tissues: 35%. • All C-atoms of cholesterol come from acetyl CoA; reducing equivalents come from NADPH • Energy to drive synthesis comes from ATP hydrolysis • Key enzyme (rate limiting enzyme) in cholesterol synthesis is HMG CoA reductase
Cholesterol synthesis • First three acetyl CoA forms HMG CoA • HMG CoA reductase catalyzes the rate limiting (regulated) step of the pathway, formation of mevalonic acid from HMG CoA and 2 NADPH
Decarboxylation of mevalonic acid forms isopentyl-pyrophosphate (IPP, 5-C unit). • Condensation of two IPP forms geranyl PP (GPP, 10-C) • Condensation of GPP and IPP forms farnesyl PP (FPP, 15-C). • Condensation of two FPP forms squalene (30-C). • Squalene becomes cyclized lanosterol, and then cholesterol
Regulation of cholesterol synthesis • Regulation of cholesterol synthesis via : • feedback inhibition of HMG CoA reductase by cholesterol • cholesterol inhibits transcription of HMG CoA reductase gene • Inhibit by drugs, such as Compactin and Lovastatin. R= H: compactin R= CH3: lovastatin
-- hormonal regulation of HMG-CoA reductase • glucagon leads to phosphorylation: inactivate the enzyme • insulin favors dephosphorylation: activate the enzyme
Metabolism of Bile acids • Formed from cholesterol in the liver • Rate limiting step is the conversion of cholesterol to 7-alpha cholesterol by 7-a-hydroxylase • Utilized during digestion of fats (act as detergents)
Bile acids & salts • Before leaving the liver, bile acids are conjugated in amide linkage to glycine (glycocholic acid) or taurine (e.g. taurochenodeoxycholic acid) • These compounds are more fully ionized at neutral pH (carboxylate and sulfate, with low pKa) and are better detergents
Conversion of cholyl-CoA to glycocholic acid Glycocholic acid Glycochenodeoxycholic acid
Conversion of cholyl CoA to taurocholic acid Taurine Taurocholic acid Taurochenodeoxycholic acid
Secondary bile acids • Bacteria in the intestine can remove glycine and taurine • They can also modify bile acids to form secondary bile acids (minus one -OH group, e.g., deoxycholic acid, lithochoic acid)
Glycocholic acid Deoxycholic acid Taurocholic acid
Glycochenodeoxycholic acid Lithocholic acid Taurochenodeoxycholic acid
About bile acids • Cholic acid is the bile acid found in the largest amount in bile • Cholic acid and chenodeoxycholic acid are referred to as primary bile acids • Bile acids are converted to either glycine or taurine conjugates (in humans the ratio of glycine to taurine conjugates is 3:1) • Bacteria in the intestine can remove glycine and taurine. They can also modify bile acids to form secondary bile acids (minus one -OH group, e.g., deoxycholic acid, lithochoic acid).
Function of bile acids • Aid in digestion and absorption of dietary fat: emulsify fats due to detergent activity • Stimulate the action of pancreatic lipase • Stimulate intestinal motility • Keep cholesterol in solution (as micelles)
Mixed micelle formed by bile acids, triacylglycerols and pancreatic lipase • Detergent character of bile salts is due to the hydrophobic-hydrophilic nature of the molecules
Bile acids are efficiently recycled Enterohepatic circulation: • Bile acids are efficiently reabsorbed in the intestine and returned via the portal vein to the liver for reuse (enterohepatic circulation) • Of 15-30 g of bile acids secreted/day, only 0.5 g are lost in feces (i.e., 0.5 g of cholesterol is excreted)
Cholelithiasis If more cholesterol enters the bile than can be excreted, cholesterol may precipitate/ crystallize in the gall bladder leading to gallstone disease • Causes: • severe ileal disease • obstruction of the bile duct • severe hepatic dysfunction • excessive suppression of bile acid synthesis
Lipoproteins and Atherosclerosis LDL: Risk factor for atherosclerosis HDL: Protective factor for atherosclerosis
Atherosclerosis • hardening of the arteries due to the deposition of atheromas • caused by the deposition of cholesteryl esters on the walls of arteries • atherosclerosis is correlated with high LDL and low HDL Author: Sukhinder C. Kaur 572 pages, Springer; $139.00
Lipoproteins and atherosclerosis • The endothelium in the arterial wall becomes more permeable to lipoprotein and allows migration of cells to the underlying layer (intima). • LDL penetrate the vascular wall and deposit in the intima, where they undergoing oxidation to become oxidized LDL (OxLDL). • Oxidized LDL stimulate endothelial expression of some adhesion molecules. • Adhesion molecules attract monocytes, which enter the wall and transform into macrophages.
Macrophage take up oxidized LDL, when overload with lipid, become “foam cells”. • Conglomerate of foam cells form fatty streaks or yellow patches visible in the arterial wall. • Dying foam cells release lipid that form lipid pool within the arterial wall. Foam cells
Surrounding smooth muscle start to secrete a range of small peptides, which stimulate smooth muscle cells to proliferate and to migrate toward the lumen side of the arterial wall. • In the same time, smooth muscle cells start synthesizing extracellular matrix, such as collagen. • Relocated smooth muscle cells, collagen-rich fibrous tissue, macrophages all together form a “Cap” that cover the lipid pool. This is a matured atherosclerotic plaque.
Fibrous cap Thrombus Lipid core • The plaque protrudes into the arterial lumen, grows slowly over years, and finally obstruct the artery. This decreases blood flow in the affected vessel. • Rupture or ulceration of fibrous cap rapidly leads to thrombosis and obstruct the artery.
HDL is Protective • HDL prevent foam cell formation • HDL inhibits oxidative modification of LDL • HDL inhibits expression of adhesion molecules
Improving Your Levels http://mayoclinic.com/health/high-blood-cholesterol/DS00178/DSECTION=9 Exercise Improved diet Maintain a healthy weight Quit smoking Possibly cholesterol drugs
Diet Reduce your intake of fats and cholesterols. Increase your intake of fruits and vegetables. Add more fiber. Eat low-fat or fat-free dairy products. Avoid eating too many calories.
Exercise 30 minutes a day 4+ times a week
Cholesterol Drugs Talk to your doctor, and follow his/her advice.