Download

1 / 57
670 likes | 1.05k Views
Q Fever. Coxiella burnetti. Overview. Organism Transmission Epidemiology Disease in Humans Case Studies Disease in Animals Medical Surveillance Laboratory Procedures Respiratory Protection (N95) Emergency Procedures Prevention and Control. Organism. The Organism. Coxiella burnetii

E N D
Q Fever Coxiella burnetti
Overview • Organism • Transmission • Epidemiology • Disease in Humans • Case Studies • Disease in Animals • Medical Surveillance • Laboratory Procedures • Respiratory Protection (N95) • Emergency Procedures • Prevention and Control
The Organism • Coxiella burnetii • Obligate intracellular, gram negative bacterium • Forms spore-like structures • Highly resistant to heat, drying, & some disinfectants • Can survive for months in dust & feces particles • Killed by pasteurization • Exists in two antigenic phases • Phase 1: virulent-infected animals/humans and in nature • Phase 2: less pathogenic- found after multiple lab passages in eggs or cell cultures
Q stands for Query • Discovered in 1937 in Queensland, Australia (slaughterhouse workers) • 1938- Montana, USA (isolated from ticks) • Outbreaks • Largest outbreak 2007-2010 more than 4,000 cases in the Netherlands; required euthanizing 50,000 goats • 2011- Northwestern US-involved 21 goat farms and resulted in 20 human infections • Military troops • In areas with infected animals • Cities and towns • Downwind from farms • Near roads traveled by animals
Transmission • Inhalation (most common) • Dust, droplets • Birthing fluids/amniotic fluid/placenta • 109 bacteria released per gram of placenta • Urine, feces, raw milk • Direct or indirect contact with infected animal • Contaminated surfaces, equipment, bedding, etc • Arthropods (ticks) • Person to person transmission is rare
Epidemiology • Worldwide • Except New Zealand • Primary reservoirs • Ruminants-Sheep, cattle, goats • Pregnant females, fetuses, females that have just delivered/aborted, newborns • Cats, dogs, rabbits • Birds • Reptiles • Wildlife species: moose, white-tailed deer, black bears
Epidemiology • Who’s at risk? • Farmers • Veterinarians • Meat processors/ abattoir workers • Laboratory workers/animal laboratory workers • Immunocompromised • Pregnant women
Q Fever in the U.S.: *CDC 2011
Human Disease • Incubation: 2 to 4 weeks • Disease • 50%-Asymptomatic • Acute • Chronic
Acute Infection • Flu like symptoms: high fever (up to 104-105◦F), headache, sore throat, vomiting, nausea, fatigue • Pneumonia with mild cough (50%) • Less common • Hepatitis, myocarditis, central nervous system complications • Self-limiting-38% • >50% asymptomatic • 2-4% require hospitalization • <1% mortality rate
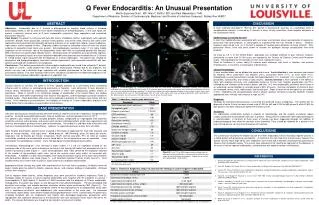
Chronic Disease (> 6 months) • 1-5% of acutely infected individuals • Pre existing heart conditions, pregnant women, immunocompromised • Endocarditis (60-70%) • Other • Aortic aneursyms • Osteomyelitis • 50% relapse rate despite antibiotic therapy • Mortality rate >50% • Endocarditis- fatality rate 25-60% if untreated
Risk to Pregnant Women • Most asymptomatic (98%) • Transplacental transmission • Reported complications • Premature birth • Low birth weight • Miscarriage • Placentitis • Greatest risk during 1st trimester
Diagnosis • Serology (most common method) • IFA, CF, ELISA, microagglutination • DNA detection methods • PCR • Isolation of organism • Not recommended • Poses risks to laboratory personnel • BLS 3- Select Agent
Treatment • Treatment –ideal to begin first 3 days of illness • Acute disease • Doxycycline (2-3 weeks) • Chronic disease • Doxycycline and hydroxychloroquine (~18 months) • Immunity • Long lasting (possibly lifelong)
Dairy Farmer Case • 2001 • Dairy Cow Farmer (Georgia) • Sudden onset of flu-like symptoms: fever, chills, cough • Diagnosed as influenza • 2 weeks later presented to emergency room-again diagnosed as flu
Dairy Farmer Case • Referred to infectious disease specialist • Tested positive for Q fever (phase II) • 5 day course anitibiotics-symptoms resolved in 2 weeks • Epidemiology • No recent animal births on his farm • Two beef cattle herds of approximately 35 animals each were across the road • 2 out of 14 tested were positive for Q fever MMWR 10/2002
Poker Player’s Pneumonia March 5-16, 1987 Nova Scotia, Canada • 12 individuals who often played poker together were infected with Q fever. • Symptoms: headache, pneumonia, cough • Cat gave birth to kittens, 1 stillborn on 2/14/87 in the room where poker was played • Direct contact not required
Military Personnel • Reports of US military personnel deployed in Iraq and Afghanistan, including some without any known animal exposure. • Since 2003, more than 200 cases of acute Q fever have been reported among US military personnel deployed to Iraq. • May 2010- CDC issued a health advisory warning about the potential of Q fever among travelers returning from Iraq and the Netherlands.
Animal Disease • Sheep, goats, cattle • Often asymptomatic • Reproductive failure • Abortions • Stillbirths • Low birth weight • Weak newborns • Infertility • Carrier state • Other animal species • Dogs, cats, horses, rabbits, birds
Morbidity and Mortality • Prevalence information is limited • Endemic areas • 18 to 55% of sheep with antibodies • 82% of dairy cattle with antibodies • Death is rare
Prior to working with sheep • The following should contact the University Employee Occupational Health Clinic (UEOHC) for a medical screening/risk assessment: • Immunocompromised individuals and those with pre-existing heart valve conditions are at higher risk of infection and should be fully informed of the increased risks. • Pregnant women or women who are considering becoming pregnant should also be fully informed of the increased risks. UEOHC Monday- Friday (8:30am-4:30pm) 919-966-9119
Exposure Procedures • Percutaneous exposure (needlesticks, cuts, animal bites or scratches) • Remove contaminated gloves and if possible, allow the wound to bleed freely for a minute. • Wash the wound with soap and water for 5 minutes and apply sterile gauze or a bandage, if necessary. • Remove protective lab clothing and follow reporting procedures.
Exposure Procedures • Mucous membrane exposure. • Rinse tissue surface with copious amounts of water. • Eyes will be irrigated for at least 5 minutes using the emergency eye wash station. • Remove protective lab clothing and follow reporting procedures. Inhalation exposure Remove protective lab clothing and follow reporting procedures.
Reporting Exposure Events • Employees must be seen by UEOHC 919-966-9119 (M-F, 8:30am-4:30pm) for treatment and documentation of exposure immediately following the incident during work hours or on the next business day if the incident happens after hours. • If the injury required first-aid after hours, go to the UNC Hospital Emergency Room. • An Exposure Incident Report (Form 19) must be completed by the employee at UEOHC. • EHS will also complete a report that includes how the incident was addressed.
Reporting Signs and Symptoms of Exposure • Employees experiencing any of the symptoms associated with exposure (even without an identified exposure incident) must report it to the PI, UEOHC, and EHS. • If you have worked in the lab within the last two weeks of experiencing any of the symptoms associated with Q fever, report it to the PI, UEOHC, and EHS.
Post Exposure Treatment/Testing If prophylactic antibiotic treatment is considered appropriate by clinic or ER medical staff, doxycycline is generally given for 2-3 weeks (acute) or doxycycline and hydroxychloroquine for at least 18 months (chronic) unless otherwise contraindicated.
Laboratory Procedures PPE Biohazardous Waste
Laboratory Standard Operating Procedure • Safe handling procedures, including: • Personal protective equipment • Engineering controls • Reporting injuries and occupational exposures • Reviewed annually by PI, EHS, IBC, and employees
Laboratory/Animal Housing Entry • Don PPE • Latex/nitrile gloves • Tyvek (disposable jumpsuit) • Bonnet • Shoe covers • Eye protection (lab) • N95 or PAPR
Laboratory/Animal Housing Exit • Wash hands after removing gloves and prior to leaving area. • Minimize the creation of droplets, splashes, aerosols, and dust • Decontaminate work surfaces immediately following spills, elimination from sheep
Sharps Precautions • Needles should only be used when there is no other alternative • Injection of animals and blood draws • Do not break, bend, re-sheath or reuse syringes or needles. • When needles are required, safe needle devices should be used • Passive safety features recommended
Needles & Sharps Precautions Contaminated sharps must be placed in hard walled plastic containers labeled with the biohazard symbol as shown. When the container is no more than 2/3 full, place autoclave indicator tape over the biohazard symbol in an “X” pattern as shown. Containers must be placed in biohazard bag prior to autoclaving.
Biohazardous Waste • All biohazardous waste (including liquids) must be autoclaved prior to disposal. • Place waste in autoclave bags. • Autoclave tape over biohazard label. • After treatment, seal bags with tape. • Place in lined Rubbermaid container. Autoclaves must be tested weekly with a bioindicator to insure proper function.
Respiratory Protection Program Requirements29 CFR 1910.134 • Procedures for selecting respirators for use in the workplace. • Medical evaluations of employees required to use respirators. • Fit testing procedures for tight-fitting respirators. • Procedures and schedules for cleaning, disinfecting, storing, inspecting, repairing, discarding, and otherwise maintaining respirators.
Respiratory Protection Program Requirements29 CFR 1910.134 • Training of employees in respiratory hazards to which they are potentially exposed during routine and emergency situations. • Training of employees in the proper use of respirators, including putting on and removing, any limitations on their use, and the maintenance of the respirator. • Procedures for regularly evaluating the effectiveness of the program.
Q Fever:Respiratory Protection • PAPR respirators or N95 masks are required to enter the animal housing area and laboratory • Annual training and respiratory clearance required (clearance is done at the UEOHC) • Annual fit testing for N95 is required.
Medical Surveillance • Required to determine the employee’s ability to use a respirator. • Medical evaluation can be conducted through a questionnaire, and then through a medical examination if a positive response is received for certain questions. • There is a physiological burden on employees that varies with the type of respirator worn, the job, the workplace conditions in which the respirator is used, and the medical status of the employee.
Biohazardous Spills • Animal bedding • Sheep urine, fecal material, blood
Spill procedures are posted in the facility. • Where is the spill kit located in your facility?
Spills (Sheep body fluids, blood) • Secure sheep. • Assess personal exposure and remove & replace any contaminated gloves, coveralls or shoes, • Use the disinfectant solution located in the facility or spill kit to carefully dilute the spill from the outside edges. • Use an absorbent pad or paper towel to collect the spill. • Dispose in biohazard bag. • Spray and wipe the area once more with approved disinfectant. • Discard of paper towels and contaminated PPE in biohazard bag. • Wash your hands and don fresh PPE. • Sharp objects must be handled by mechanical means (forceps, dust pan and squeegee).