Download
1 / 43
430 likes | 540 Views
Audit Your Practice. Presented By:. Larry Elisco, CPA, ABV, CCS-P Member Weltman Bernfield LLC 847.941.0245 lelisco@weltmanbernfield.com. AAOS Disclosure Information. My disclosure is in the Symposium Syllabus and in the AAOS database.

E N D
Presented By: Larry Elisco, CPA, ABV, CCS-P Member Weltman Bernfield LLC 847.941.0245 lelisco@weltmanbernfield.com
AAOS Disclosure Information • My disclosure is in the Symposium Syllabus and in the AAOS database. • I have no potential conflicts with this presentation.
Auditing • The Definition of Auditing*: “An official examination and verification of accounts and records, especially of financial accounts” *Dictionary.com
Auditing – Cost vs. Benefit • Benefits • Internal control/safeguarding of assets • Educational to physicians • Performance measurement for employees • Possible support in the event of an OIG investigation (attorney client privilege must be considered) • Costs • Significant up front work as well as ongoing time performing testing and maintaining records of results
AUDIT ISSUES TO BE ADDRESSED • Design of Accounting System • Contract Documentation • Compliant Reimbursement • Collection Performance • Safeguarding of Assets • Independent Review of Coding
4 Areas of Focus • Billing and Reimbursement • Contracts • Adjustments • Accounts receivable • Aging • Collection performance • Financial Auditing and Controls • Coding
Auditing Process • Documentingsystem design • Identify processes and parties responsible for those processes • Test compliance • Review a sample of transactions during a specified period • Review of results by Management
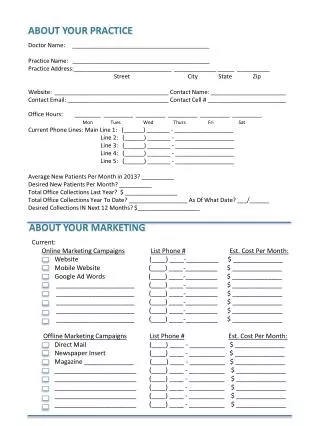
Documentation and Evaluation of Processes • Develop Job Descriptions • Define Functional Responsibilities • Daily • Weekly • Monthly • Evaluate Opportunities for Errors or Irregularities • Consider implementing checks & balances Source: microsoft.com/images
Example of Functional Responsibilities The Billing Manager is responsible for the following: • Design of procedural systems and manuals • Monitoring accounts receivable including approval of adjustments • Monitoring accuracy of billing and reimbursement • Managing staff responsible for billing and reimbursement • Reviewing medical coding as documented by doctors • Preparing practice management reports as needed • Reporting to management on effectiveness of billing and reimbursement procedures • Preparing end of day reports and making bank deposit
Example for Implementing Checks and Balances • Practice Manager prepares the end of the day deposit from the PM system. • Practice Manager makes the deposit at the bank. • Practice Manager has the ability to make adjustments to patient balances in the PM system. • Practice Manager then has the ability to divert funds to a personal account and write off the balance as a bad debt.
Example for Implementation of Checks and Balances(continued) • In this case, someone other than the Practice Manager should be making the bank deposit and completing the end of day report. • Preference would be having a physician making the bank deposit after reviewing the end of day report and deposit slip. Source: microsoft.com/images
Billing and Reimbursement • Review written procedures in place for recording and approving adjustments (or have procedures developed) • Using payor contracts, document the details of the reimbursement terms for each contract in place for the practice and maintain in a centralized location (example to follow) on the practice’s network • Include the basis for reimbursement (generally a formula utilizing the percentage of the Medicare fee schedule for each CPT code)
Billing and Reimbursement • In some cases payment is made on the basis of the payor’s usual and customary reimbursement for a given CPT code, particularly for out-of-network payors where no contractual relationship exists • In those cases it may be necessary to “reverse engineer” the reimbursement by comparing the reimbursement to the Medicare fee schedule to arrive at the formula
Billing and Reimbursement • The payor may only be willing to provide reimbursement on a limited number of CPT codes per contact, making it difficult to establish comprehensive fee schedules for a given payor. • Focus on the CPT codes most frequently used by the practice Source: microsoft.com/images
Example of Contract Details Source: Courtesy of Larry Elisco, CPA
Billing and Reimbursement • Obtain the population of encounters paid in a given period (monthly, quarterly, annually). For each encounter: • Stratify (segregate into groups) the sample by payor and by responsible biller • Select an aggregate sample of 100 transactions* • Obtain Explanation of Benefits statements for the encounters sampled • Follow each transaction through the cycle documenting exceptions such as denials, bundling, payments less than contract *generally considered a reasonable annual sample size (per group of accounts) without doing a statistical sample
Billing and Reimbursement • Trace the reimbursement from each sample to the contractual terms for the given payor • Quantify the exceptions and document the cause, e.g. bundling of procedures, denials for medical necessity • Develop a list of denial reasons and quantify by payor and overall • Document process for appealing on claim denials and note for each sample if process was adhered to • Document result of appeals process for each sample
Billing and Reimbursement • Quantify the results of testing • List error rate for sample • List the result by payor to establish a pattern of improper reimbursement and/or denials • Maintain statistics on a cumulative basis for a given period
Example - Testing Results Source: Courtesy of Larry Elisco, CPA
Example – Summary of Testing Results • In September 2012, The practice incurred an error rate of .91% on the items tested. • BCBS bundled procedures for ________ which are being appealed • Medicare denied _______ because of medical necessity, we have an ABN from the patient and will make it their responsibility • Aetna bundled ______ which was a billing error and is being written off as a contractual adjustment
Billing and Reimbursement- Adjustment Report • For the entire population of collections for a given period, develop a report that lists all adjustments sorted by payor and then CPT code • Adjustments should be analyzed for outliers where the adjustment within a payor and CPT code differs from the population
Report on Adjustments • Outliers over a certain amount require investigation and explanation • Quite often the outliers are the result of modifiers to a CPT code, which are generally acceptable. • Other causes for outliers could be • Denials • Bundling • Payor error • Bad debt write-offs • Irregularities such as writing off co-pays where employee is stealing • CCI Edits
Report on Adjustments Source: Courtesy of Larry Elisco, CPA
Adjustment Report-Summary of Results • BCBS – Johnson – Reimbursement error, being appealed • UHC – Morgan - denial due to demographic error in address, being rebilled • Medicare – reimbursement error being appealed
Accounts Receivable • Review written procedures in place for accounts receivable collection (or have procedures developed) • Develop a checklist of procedures to be performed in accounts receivable collection efforts Source: microsoft.com/images
Accounts Receivable • Obtain end of month accounts receivable aging and identify balances greater than 60 days old • Where multiple employees are assigned to a range of balances (e.g. alphabetical assignments) stratify the balances so that each employees work is audited. • Review collection process for each item in excess of a nominal amount such as $500 and retain documentation • Based on balances sent to collection, compute monthly bad debt expense for each employee and quantify as a percentage of collections • EG – billed X wrote off Y for month and cumulatively for the year to date
Accounts Receivable • Establish a grading system where bad debts as a percentage of collections equal a grade for purposes of employee evaluation • 0% to .5% = Outstanding • .6% to .8% = Good • .9% to 1.0% = Acceptable • > 1% = Unacceptable • Maintain testing results for the period being tested and cumulatively report over given periods, such as month and year to date
Accounts Receivable • Document the results of each monthly review, scan and save to practice computer network • Reference prior month’s documentation each month when discussing current status Source: microsoft.com/images
Case Study Accounts Receivable • Radiology practice consisting of 4 physicians was disbanding, we were engaged to handle the financial affairs of the winding down of the practice • We immediately noted accounts receivable balances of approx. $1.5 million that were more than one year old (net was approximately $900,000) • When this was raised with the physicians they didn’t understand what accounts receivable were and never saw an accounts receivable aging.
Case Study Accounts Receivable, (continued) • Subsequent discussions with the billing service responsible for collections became hostile, however did yield quite a bit of action. • The practice ended up collecting approximately 40% of the old balance and writing off over $500,000 of net accounts receivable
Financial Auditing and Controls • For a given period, obtain a check register (listing of all checks and disbursements including automatic bill payments and wire transfers) • Scan the list to determine if any disbursement to a vendor appears unusual • Select a sample of transactions and trace the sample to: • The actual check to ensure the payee matches what is reflected on the check register (Quickbooks can be altered) • The bank statement to ensure the amount cleared agrees to the check register
Financial Auditing and Controls • For a given period, obtain all end of day reports for the practice • Trace the total for each day report to the cash deposit reflected in the practice’s general ledger (often Quickbooks) • Trace the amount deposited to the bank deposit slip • Trace the amount on the bank deposit slip to the bank statement • Any variances require investigation and explanation
Financial Auditing and Controls • For a given period, obtain the payroll journal for the period • Scan the list to ensure all employees reflected on the list are actual employees • For new and selected existing employees, review personnel files to ensure that proper documentation is in place such as: • W-4 forms • Copy of a form of Identification (driver’s license) • Election forms for retirement plans
Financial Auditing - Quickbooks • Quickbooks is the most common accounting package used by medical practices. • Transactions recorded in Quickbooks can be changed/altered at a later date. • The payee on large payments made to vendors like the IRS, medical suppliers or employees can be changed after the fact • Discovery of this type of embezzlement may take an extended period of time
Actual Incident of Embezzlement • Practice processes payroll internally, does not use an outside service • Bookkeeper has a gambling problem, makes out a series of checks to a fictitious company she owns and changes the payee in Quickbooks to the IRS • Bookkeeper also opens the mail, and destroys tax notices received by the practice on the shortfalls • Practice loses over $250,000 which can’t be recovered
Actual Incident of Embezzlement(continued) • This could have been prevented by: • Comparing the payee reflected in Quickbooks check register to the actual cleared check from the bank (auditing) • Using an outside payroll service • Having the mail opened by someone other than the bookkeeper (segregation of duties) Source: microsoft.com/images
Financial Reporting on Payor Performance • Prepare these reports • Payor mixfor a given period and compared to other periods • Average reimbursement rate as a percentage of Medicare by payor • Average days to collect charges by payor for a given period of time and compare to prior periods
Coding • For a given period select a sample of Encounters using CPT Codes (e.g. office visits) • Stratify the sample by physician (assuming group practice) • Obtain op reports or electronic ticket (superbill) for the charge • Physician or coder that did not perform the service should code the procedure based on the SOAP notes or op report • Independent coding should then be compared to actual coding for procedure • Results should be reported on and differences investigated and discussed with physician
Coding • For a given period, list CPT codes by physician (group practice) • Quantify (list) in a graphical format the codes used by each physician and compare to the overall coding results for the practice • Physicians coding significantly different from their peers and their practice as a whole, either over or under, should be discussing their coding practices with the group
Coding Patterns for Dr. Smith Source: Courtesy of Larry Elisco, CPA
Checklists • Handouts are checklists for: • Billing and Reimbursement • Accounts Receivable • Financial Auditing and Reporting • Coding
Thank You! Larry Elisco, CPA, ABV, CCS-P Member Weltman Bernfield LLC 847.941.0245 lelisco@weltmanbernfield.com