Download
1 / 32
380 likes | 583 Views
Dr Sarah J Johnson Consultant Cyto/histopathologist Newcastle upon Tyne. Molecular testing of thyroid nodules. This talk. Overview of molecular abnormalities in thyroid lesions Potential value Our own work.

E N D
Dr Sarah J Johnson Consultant Cyto/histopathologist Newcastle upon Tyne Molecular testing of thyroid nodules
This talk • Overview of molecular abnormalities in thyroid lesions • Potential value • Our own work
Overview of molecular abnormalities(Nikiforov YE, Modern Pathology 2011;24:S34-43;Bhaijee F & Nikiforov YE. EndocrPathol 2011;22:126-133.Nikiforova MN & Nikiforov YE. Thyroid 2009;9:13511361. • Recent dramatic increase in understanding of molecular biology of thyroid cancer • Main four • BRAF and RAS point mutations • RET/PTC and PAX8/PPARγgene rearrangements • Others • PI3K/AKT signalling pathway - PDC • TP53 and CTNNB1 mutations – PDC, ATC • TRK rearrangement – PTC but rare
Nikiforov Arch Pathol Lab Med 2011;135:569-77 Bhaijee & Nikiforov Endocr Pathol 2011;22:126-33 Nikiforova & Nikiforov Thyroid 2009;19(12)1351-61 Prevalence of mutations
BRAF point mutations • Intracellular effector of MAPK signalling cascade • Most V600E → activate BRAF kinase, stimulate MAPK pathway → tumourigenic for thyroid cells • 1-2% - other mutations egK601E • BRAF V600E mutation • quite specific for PTC and related tumour types • 60% classical PTC • 80% tall cell variant PTC • 10% FVPTC • 10-15% PDC • 20-30% ATC • NOT in FC, MTC or benign nodules • early in pathway
BRAF - clinical and prognostic valueMelcket alThe Oncologist 2010;15:1285-93; Yip et al.Surgery2009;146:1215-23; Xing et al J ClinOncol2009;27:2977-2982. • Associated with aggressive tumour characteristics (V600E only) • ETE, multicentricity, advanced stage, LN+, distant metastases, recurrence, persistence, re-operations, tall cell morphology, lymphovascular invasion, suspicious USS features • especially >65 yrs • Independent predictor of treatment failure, tumour recurrence, tumour-related death • Even in microPTC – associated with poorer clinicopathological features (eg ETE, LN+) – exciting because management debated • May relate to • tendency to de-differentiate • reduced ability to trap radio-iodine • less responsive to TSH suppression
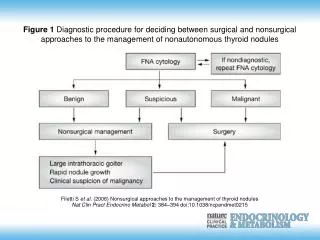
BRAF – diagnostic value in cytologyAdeniran et al Thyroid 2011;21(7):717-23. Bentzet al Otolaryngol Head and Neck Surgery 2009;140:709-14 • BRAF mutation strongly correlates with PTC, independent of cytology • Improves accuracy, specificity and PPV for PTC • Specificity and PPV for PTC with BRAF-positivity = virtually 100% • Mixed results for sensitivity & NPV, can be low • Helpful in identifying PTC in “indeterminate” cytology samples • Could use to change management decision positive Total thyroidectomy +/ level VI LNs Indeterminate cytology BRAF test negative Diagnostic hemithyroidectomy
BRAF –accuracy in cytology • 6 false positives for malignancy with BRAF analysis • 1 case in Korea – indeterminate cytology, BRAF-positive → histology of “atypical nodular hyperplasia” • 5 when ultrasensitive testing used, not positive on repeat testing • Recent meta-analysis – BRAF testing in 2766 samples • 581 BRAF-positive → 580 were PTC (some with benign cytology) • rate of malignancy for BRAF-positivity = 99.8% • frequency of indeterminate cytology in BRAF-positive samples = 15-39% • Various techniques possible but need to avoid ultrasensitive detection and methods that are not well validated → may risk false positives • BRAF detection in cytology also predicts aggressiveness • BRAF-negativity with indeterminate cytology does not eliminate need for diagnostic hemithyroidectomy
BRAF –therapeutic value • Predicts aggressiveness →maybe consider more aggressive treatment, more frequent follow-up, but maybe not enough to act on yet • Therapeutic target - BRAF inhibitors eg sorafenib
RAS - point mutations • Family includes HRAS, NRAS, KRAS • Propagate signals along MAPK and other signalling cascades • Most frequent mutations in thyroid • NRAS codon 61 • HRAS codon 61 • Found in • 10-20% PTC – mostly FVPTC • 40-50% FC • 20-40% FA – but ?precursors for FC • some hyperplastic nodules but clonal so ?neoplasm • less in oncocytic tumours
RAS - point mutations • Prognosis • some association with dedifferentiation and worse outlook • but also associated with eFVPTC – indolent behaviour • Finding RAS mutation in thyroid nodule • strong evidence for neoplasia • but does not establish diagnosis of malignancy • RAS mutation in cytology • PPV for malignancy 74-88% • helpful when cytology difficult such as FVPTC
RET/PTC gene rearrangements • RET highly expressed in C cells, not follicular cells • But activated by RET/PTC rearrangement • 11 types, RET fusion to different genes • Commonest in thyroid cancer - RET/PTC1 & RET/PTC3 • All fusions activate MAPK signalling pathway • Variation in expression – needs to be “clonal”, ie majority • ClonalRET/PTC - reasonably specific for PTC • 10-20% PTC in adults • 50-80% PTC after radiation exposure (RET/PTC1 – classical PTC, RET/PTC3 – solid type PTC) • 40-70% PTC in children and young adults • Non-clonalRET/PTC – no diagnostic implications
RET/PTC- prognosis and diagnosis • PTC with RET/PTC - younger age, classical PTC histology, high rate LN metastases • But varied views on overall prognostic value • Detection of clonal RET/PTC = strong indication PTC • Histology – not useful because classical so diagnosis clear • In FNA – can improve pre-operative diagnosis PTC but can have false positives
PAX8/PPARγgene rearrangement • Fusion between PAX8 gene and perioxisomeproliferator-activated receptor (PPARγ) gene • Causes over-expression of PPARγprotein • Found in • 30-40% conventional FC • less often in oncocytic carcinomas • 5-38% FVPTC • 2-13% FA – often thick capsule, ?pre-FC or misdiagnosed • Often - younger age, smaller tumour, more frequent vascular invasion • Detection in histology not diagnostic of malignancy but should prompt exhaustive search for capsular or vascular invasion • Detection in FNA – typically malignant but numbers low
Gene expression profilesBorup et al Endocr-Related Cancer 2010;17:691-708. Maenhautet al ClinOncol2011;23:282-288. Ferrazet al ClinEndocrinolMetab 2011;96(7):2016-2026 • mRNA • no ideal marker of PTC • lack of markers to distinguish FC from FA • slight difference between radiation-induced PTC and not • ?can measure different background susceptibilities to radiation • microRNAs • easier to extract from FNA than mRNA • possible future diagnostic potential • PTC & FC have different profile to normal thyroid
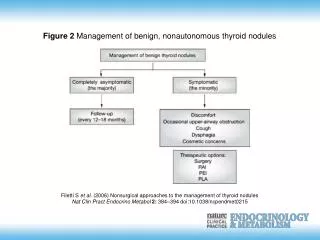
Review of 20 studies of genetic testing Ferrazet al ClinEndocrinolMetab 2011;96(7):2016-2026 • Highest sensitivity with panel of markers • BUT more FP with panel than with single marker • Best if done on same material as used for cytology, not extra • Suggest Indeterm-inate cytology Panel of markers Negative group Malignancy risk down from 20% to 8-10% miRNA Cohort with 3% malignancy risk ?follow up with USS + repeat FNA
Sample in special preservative solution → panel of 7 molecular markers Commercially available kits – USA
Sample → cytopathology → inadequate, benign or malignant report indeterminates → gene expression Commercially available kits – USA
Our own work in Newcastle • Initial project • Current BRAF pilot
Initial project – BSCC presentation 2011S. Hardy, U.K. Mallick, P. Perros, S.J. Johnson, A. Curtis and D Bourn Aim: to set up and validate assays for detection of molecular markers in thyroid samples Retrospective – archival histology then cytology Panel of markers: • BRAF codon 600 • HRAS codon 61 on extracted DNA • KRAS codons 12/13 (melt curve analysis) • NRAS codon 61 • RET/PTC rearrangements on extracted RNA • PAX8/PPARγrearrangements (RT-PCR-based assays)
Example data – NRAS codon 61 WT CONTROL CODON 61 (Q61K) CONTROL WT WT Q61K WT Q61K
Results – point mutations on thyroid histology cases • 32 cases (patients), 36 blocks • 6 non-neoplastic nodules 0/6 0% • 5 follicular thyroid adenoma (FA) 0/6 0% • 5 follicular thyroid carcinoma (FC) 1/5 20% (NRAS codon 61) • 7 papillary thyroid carcinoma (PTC) 1/6 17%(BRAF v600E) • 4 “aggressive” PTC (aPTC) 4/4 100% (BRAF v600E) • 3 poorly differentiated carcinoma (PDC) 1/3 33% (NRAS codon 61) • 1 SCC 1/1 100%(NRAScodon 61) • 1 metastatic strumaovarii 1/1 100%(NRAS codon 61) • ie. pattern as expected • Concordance between different blocks from same tumour
Results – point mutations on cytology slides Cases with molecular result available on histology: NNN 2 cases, 4 slides 1/3 50% cases (NRAS codon 61) FA 1 case, 1 slide 0/1 0% FC 4 cases, 7 slides 2/6 50% cases (1 NRAS, 1 HRAS) PTC 2 cases, 6 slides 1/3 17% (NRAS codon 61) aPTC 3 cases, 9 slides 4 tumour 3/3 100% (2 BRAF V600E, 1 HRAS codon 61) 5 LN/bed 1/3 50% cases (HRAS but in neg LN) PDC 1 case, 2 slides 0/2 0% Cases with no molecular result available on histology: Thy4 (histol = FA) 0/1 0% Thy3 (histol = FC) 0/1 0% Thy3f (histol = FC), 4 slides 2/2 100% (NRAS,HRAS)
Results as cancer patients 23 cancer cases • 21 molecular results on histology • 9/21 mutations • 5 of 9 had molecular tests on cytology: 2 fails, 3 positive matches • 2 no molecular result on histology • 1/2 mutation on cytology ie. cytology found mutations in 57% (4/7)
Results as mutations 13 cases with mutations (on cytology and/or histology) • 12 malignant outcome • 1 benign outcome 9 histology cases with mutations – all malignant outcomes 11 cytology slides with 12 mutations - 7 patients - 6 malignant outcomes
Results as cytology slides • 37 cytology slides • 29 thyroid, 4 LN, 4 recurrences • Most were DQ slides • Failure rate 9of 37 = 24% • 1 LBC slide (SurePath) - paired DQ worked • 2 cyst fluid only (LN met) – failed (same case histology worked) • 2 unsatisfactory slides (1 thyroid, 1 bed) – a paired US worked • 1 with lots blood & colloid – paired slide worked • 2 Thy3f • 1 Thy5
Results as cytology slides • 37 cytology slides • 24 slides with histology mutation result available • 9 in agreement for no mutation • 4 in agreement for presence of mutation • 5 discordances – mutations in cytol not histol, 4 malignant outcomes • 11 cytology pairs (2 slides from same specimen) • 4 matches – 1 fail, 1 NRAS, 2 no mutation • 7 mismatches – 3 with one fail, 2 NRAS v fail, 1 NRAS v no mutation, 1 BRAF V600E v HRAS codon 61 • 1 of 4 slides from same specimen • 2 fail, 1 NRAS & HRAS, 1 HRAS only
Conclusions from initial study • Molecular testing for DNA point mutations is feasible in stained thyroid cytology samples • PPV 92% for malignant outcome • BUT • not always successful result • not always match of cytology with cytology, or cytology with histology • can have multiple mutations in one sample and/or tumour • can have mutations in negative LN cytology sample from cancer case • can have mutations in non-neoplastic nodules • Next step – prospective BRAF testing for 12 months • Molecular testing also feasible in histology of thyroid cancers – possible future role for individualised treatment and prognostication • Mutation-specific targeted therapies?
Current BRAF Pilot • Prospective • 12 months BRAF testing on cytology reported as Thy3a, Thy3f, Thy4 and Thy5 PTC • No result to clinician, no action on result • Will then • correlate with surgical and histological outcome • assess whether BRAF result would have influenced management decision
BRAF Pilot – results so far • Tested 14 cytology slides from 13 patients • Slide types • 12 DQ – all worked, even with heavy bloodstaining • 1 ICC for Tg on destained DQ – worked • 1 SurePath LBC – failed • Outcomes • 2 BRAF V600E mutations • LN5 met PTC (histol = classical & follicular variant, pT3 pN1b) • Thyroid Thy5 PTC (histol = classical multifocal, pT1b pN1b) • 11 wild type • 7 Thy3a - 1 with histol = FA • 3 Thyf - 1 with histol = dominant nodule with contralat PTC • 1 Thy5 ATC vs MM – histol = ATC
Summary points for whole talk • Molecular testing of thyroid cytology and histology specimens is feasible in routine labs • Diagnostic aims • single stage theraeutic surgery for cancers • avoiding diagnostic hemithyroidectomies for benigns • BRAF mutation shows most promise • diagnostically, prognostically & therapeutically • Other mutations and rearrangements • diagnostically & prognostically – less predictive • Also likely future role for microRNA studies