Download
1 / 12
140 likes | 733 Views
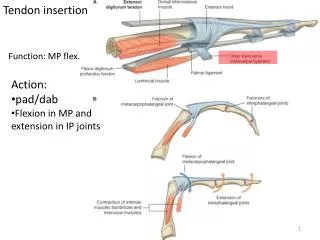
RevisionWhich structures produce flexion of the IP joints?What is the purpose of the flexor tendon sheath?What components make up the flexor sheath?How do they differ and why?What biomechanical significance does the pulley system have?How do flexor tendons receive their nutrition?How do flexo

E N D
1. FLEXOR TENDON REPAIR Judith Wood
Senior OT
October 2000
4. Adhesions absence of tendon glide
extrinsic healing
increased after infection
inflammation/oedema increases resistance to active flexion
greater strain, rerupture
disruption of tendon sheath loss of biomechanical advantage
increase of the moment arm
requiring greater excursion
infection leads to proliferation of extrinsic activity and more adhesions
alternatively breakdown of repaired structures
rerupture inappropriate stress on the repair
damage to the nutritional source
poor surgical repairAdhesions absence of tendon glide
extrinsic healing
increased after infection
inflammation/oedema increases resistance to active flexion
greater strain, rerupture
disruption of tendon sheath loss of biomechanical advantage
increase of the moment arm
requiring greater excursion
infection leads to proliferation of extrinsic activity and more adhesions
alternatively breakdown of repaired structures
rerupture inappropriate stress on the repair
damage to the nutritional source
poor surgical repair
5. Characteristics of an ideal flexor tendon repair Strickland JW.(1995) Sutures easily placed in the tendon.
Secure suture knots.
Smooth juncture of tendon ends.
Minimal gapping of tendon ends.
Minimal interference with tendon vascularity.
Sufficient strength to permit early stress.
6. The Development of Active Mobilization. Studies by Kleinert et al (1967), and Strickland and Glogovac (1980), amongst others, indicated that active movement produced greater tendon excursion than passive movement.
10. Post-operative management at Blackburn Royal Infirmary We currently follow the Belfast Regime.(Small et al.,1989)
Dorsal blocking splint with the wrist at approximately 30 degrees; MCP�s at 60 or 70 degrees and the IP joints at neutral.
Active mobilization is best begun at 3 or 4 days post op. (maybe initiated sooner depending on pain or oedema, but not later)