Download
1 / 38
760 likes | 1.62k Views
THERAPIES CIBLEES en cancérologie. Nicolas Mounier Onco-Hématologie CHU Nice – Hôpital l’Archet. Introduction. Mouvement de la cancérologie classique Identification de l’organe/tumeur initiale Diagnostic microscopique Vers cancérologie moléculaire Entité tumorale clinico-biologique

E N D
THERAPIES CIBLEES en cancérologie Nicolas Mounier Onco-Hématologie CHU Nice – Hôpital l’Archet
Introduction • Mouvement de la cancérologie classique • Identification de l’organe/tumeur initiale • Diagnostic microscopique • Vers cancérologie moléculaire • Entité tumorale clinico-biologique • Thérapeutiques ciblées 6 altérations clefs Immortalité Auto-suffisance pr croissance Insensibilité inhibiteur Résistance apoptose Angiogénèse Pouvoir métastasiant
Traitements ciblés en cours de développement en cancérologie • Les cibles => quelques exemples • Perspectives • Zoom sur les toxicités
Les cibles 1 La signalisation cellulaire 2 L’angiogenèse • Les voies de l’apoptose • Le cycle cellulaire • Les cibles épigénétiques • La méthylation du DNA • L’acétylation des histones • L’immunité anti-tumorale
P P P Ras STAT STAT STAT Raf MEK ERK TK receptors TK receptors Extracellular Membrane Jak Src PI3K Grb2 P P Cytoplasme P Src P SOS P P STAT STAT STAT Abl PDK Akt mTor p53 p70S6K p53 Gene Transcription Cell Growth Proteins translation Cell Cycle Apoptosis Apoptosis
1- La signalisation : quels niveaux de ciblage ? • Ligand extracellulaire: VEGF • Récepteur membranaire: HER 1, HER 2, CD20, IGF1, CTLA4, CXCR4 • Protéines sous membranaires :Farnésyl-transférases • Transduction intracellulaire: Voie PI3K (m-TOR) , Voie PKC (enzastaurin) • Transcription : bortezomid
Ciblage des récepteurs Par des anticorps : Rituximab, Trastuzumab, Cetuximab • Pertuzumab (HER 1, HER 2), IMCA 12 et CP 751,871 (IGF1-R) Par des petites molécules: Imatinib, Gefitinib, Erlotinib • Lapatinib (EGF-R, HER-2) • AEE 788 (EGF-R, HER-2, VEGF R2) • AMN 107 (KIT, PDGFR) • PP1 (Src, Abl) • SU 6656 (Src)
Ciblage de la transduction intracellulaire • La voie PI3K et mTOR : rapamycine, RAD 001, CCI 779 • La voie PKC : PKC 412, enzastaurin • La voie Ras : ARRAY 142 886 (ERK ½), inhibiteurs de B-Raf
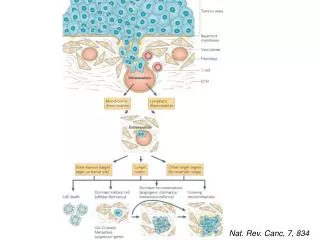
2- L’angiogenèse : quand les cibles se mélangent… • Angiogénèse :Indispensable à la survie et à la croissance tumorale • Médiée par des cytokines, des protéases et des facteurs de croissance • Ciblée par des anticorps ou des inhibiteurs de Kinases
Targeted therapy strategy • Inhibiting a single pathway (growth factor and/or receptor) • Bevacizumab – VEGF2 • Inhibiting multiple pathways (growth factors and/or receptors) • Imatinib – PDGF, KIT (receptor for the stem cell factor) • SU11248 – VEGF, PDGF, KIT, colony stimulating factor 1 receptor, and FLT-3
VEGF Family of Ligandsand Receptors VEGF- A121 VEGF- A145 VEGF- A165 VEGF- A189 VEGF- A206 VEGF- B167 VEGF- B186 PlGF- 1,2 VEGF- C VEGF- D VEGF- E Y Y s-s s-s X X NRP-1 NRP-2 VEGFR1 (Flt-1) VEGFR2 (Flk-1/KDR) VEGFR3 (Flt-4) Vasculogenesis Angiogenesis Lymphangiogenesis
Targeted therapy strategy • Inhibiting a single pathway (growth factor and/or receptor) • Becizumab – VEGF2 • Inhibiting multiple pathways (growth factors and/or receptors) • Imatinib – PDGF, KIT (receptor for the stem cell factor) • Sunitinib– VEGF, PDGF, KIT, colony stimulating factor 1 receptor, and FLT-3
KIT PDGFR ABL ABL, KIT, PDGFR Human kinome Imatinib Sorafenib (BAY43-9006) Valatanib (PTK787) Sunitinib (SU11248) Manning G et al. Science 2002; 298:1912
Perspectives • Les agents multicibles • Les combinaisons d’agents ciblés (Bévacizumab + Cétuximab ; trastuzumab + cetuximab) • Les combinaisons avec les cytotoxiques • Mais surtout, l’individualisation des choixthérapeutiques par le profil génétique des tumeurs (pharmacogénomique) et celui de l’individu (pharmacogénétique)
Zoom sur les monoclonaux Acm humanisés 1988-1991 Acm murins 1975 Acm chimériques 1984 Acm intégralement humains 1994-1999 Domaines constants VH et VL humains Rituximab, Infliximab, Cetuximab… Systèmes d’expression « display » Souris transgéniques Adalimumab CDR grafting Bevacizumab Trastuzumab… Hybridomes Muromomab
AcM thérapeutiques en 2006 Cancers du colon Cancers du rein Cancers digestifs Cancers du sein Cancer ORL Lymphomes
Rituximab : mécanismes d’action présumés rituximab CD20 FcRIIIa CD20 Effecteur cytotoxique (macrophage, NK) apoptose LYMPHOME B CD20 ADCC Souris KO FcR-g Complément C1q CDC Souris KO C1q
CHOP21 vs R-CHOP21 GELA Trial , n=399 Coiffier et al., NEJM, 2002 OS 399 patients with Diffuse large B cell lymphoma 60 to 80 years 5 yr update, Feugier et al, JCO 2005
Does Rituximab impact on survival by overcoming chemo-resistance due to Bcl-2 gene familly ? Bonavida B, Oncogene 2005
Bcl2 +, n=193 P=0.01 5 yr update, Mounier, Haematologica 2006 A Bcl2 - n=99 P=0.6 5 yr update, Mounier, Haematologica 2006 Bcl-2 DLBCL subset analysis n=292
Toxicité • Ac Monoclonaux (mab) • Relargage cytokinique • Allergie • Effets de classe : • Hémato, immunosuppression • HTA, retard cicatrisation • Inhibiteur des kinases (inib) • Nécrose tumorale • Effets de classe : • Rétention hydro sodée, T cutané • Métabolique: Hypothyroïdie, diabète • digestif • Et à long terme ?
mab VEGF Biology & Avastin effects • Mechanism of anti-VEGF efficacy • Mechanism of anti-VEGF adverse effects
mab Avastin Tolérance -Trouble de la cicatrisation ( 10 à 20% ) : - Saignement post opératoire - Retard de cicatrisation Hemorragies (4%) : Saignement muqueux , epistaxis ( 20-40 %) Tumoral ( 9%) « Terrain dépendant « ( NSCLC epidermoide) Perforations intestinales ( 1.5 à 2%) « terrain dépendant » Cancer colorectal. Cancer de l’ovaire Maladie inflammatoire intestinale ( RCH Maladie de Crohn) Diverticulose sigmoidienne Ulcere gastrique evolutif
mab Avastin Tolérance (2) -Hypertension artérielle ( 10 à 15% dont 0.7% imposant l’arrêt de Beva ) -Protéinurie (25 à 30%) -Thromboses artérielles ( 2% ) Risque augmenté chez les patients agés ( > 65 ans ) - Thromboses veineuse (?) - Asthenie - Migraine ( Toxicite aigue dose limitante en phase I 20 mg/kg ) Effets en rapport avec l’action sur la cible VEGF
mab Physiopathologie de l’hypertension -Thrombose Hypertension ( J.Yang Clinical Cancer Research): -Action du VEGF sur la « NO synthase « endotheliale -NO synthase est impliquée dans la vasodilatation et vasoconstriction et régulée par le VEGF / IL² Thrombose ( Kabbinavar JCO 2003) - Augmentation de marqueur d’activation de la coagulation ( facteur VIII Von Willebrand ) - Participation de la chimiotherapie ?
mab Physiopathologie de la protéinurie Etudes cliniques : Protéinurie 25% Etudes précliniques impact rénal ( Singe, Lapin) : Non informatives -Pas d’accumulation de Beva au niveau du rein -Pas de modification de la fonction rénale -Pas d’aggravation de l’insuffisance rénale ( modele Cisplatine ) Hypothése pour la protéinurie - Cellules mesangiales capillaires riches en VEGF ( pôle arteriel du glomérule ) - Modification de la perméabilité glomérulaire ( syndrome néphrotique ) Effet réversible sans insuffisance rénale
inib Surgical Resection of adrenal metastasis after 5 months of treatment with SU11248 Total central necrosis with no viable cancer cells Peripheral area surrounding necrosis with viable cancer cells Evidence of Tumor Necrosis Patient aged 50 Renal cell carcinoma Refractory to INF and IL2 5 previous lines of chemotherapy CT-Scan after 4 cycles
inib Tumor Necrosis SU11248 Tumor type Type of Doses (preexisting conditions) complications 100 mg q2d Renal (local recurrence) None 50 mg daily Cervix (irradiated area) Rectal fistula 75 mg daily Rectum (irradiated area) Bladder and rectal fistula UCNT (necrotic lung metastasis) Infection in necrotic areas GIST (peritoneal metastasis) Peritonitis and toxic death 100 mg daily Renal (local recurrence) None (preventive surgery)
inib ReversibleHair Depigmentation
inib KIT MAPKs + - Microphtalmia that controls the Tyrosinase gene expression Pro-melanin melanin + / - Pigmentation Sunitinib blocks KIT in animal and human c-kit antibody and SU11248 lead to depigmented gray or white hair with a decreased melanocyte proliferation and differentiation in mice
Perspectives de développement des thérapie ciblées • Au diagnostic : il existe des facteurs pronostiques => Base pour essais thérapeutiques et intégration des facteurs pronostiques biologiques • Pour le suivi : il existe méthodes statistiques => Etudes multivariées et séquentielles • La question : Bouleversement des traitements Mise en place de nouvelles stratégies - Ac monoclonaux, petites molécules - Induction, adjuvant - Consolidation, entretien