Download
1 / 32
360 likes | 950 Views
What is an Orbit? 4 5 2014. Cone-shaped Bony-walled Usually 2- one on each side of midsagittal plane Primarily sockets for eyeballs. Orbit is made up of 7 bones. Note that 4 of bones are sinus containing bones. Typical Orbit projections. Parieto-orbital-- 3 point landing (Rhese)

E N D
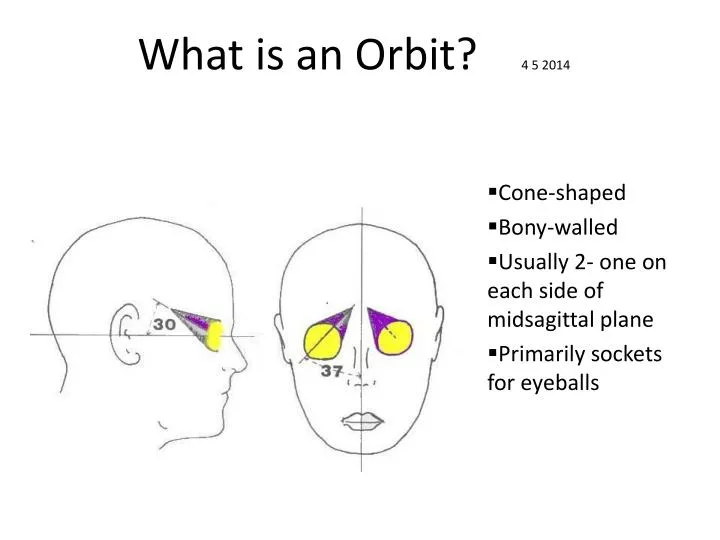
What is an Orbit? 4 5 2014 Cone-shaped Bony-walled Usually 2- one on each side of midsagittal plane Primarily sockets for eyeballs
Orbit is made up of 7 bones Note that 4 of bones are sinus containing bones
Typical Orbit projections • Parieto-orbital-- 3 point landing (Rhese) • (Orbitoparietal-- reverse Rhese) • Modified Waters (paritoacanthial) • Lateral
Optic canal (foramina)Parieto-orbital oblique (Rhese) • 3 point landing-chin,cheek, nose • center effected orbit on IR crosshairs • CR-no angle, perp. To IR • (Adjust flexion of neck to place acanthomeatal line is perp. To plane of film) • (Adjust rotation of head so midsagittal forms 53 deg. Angle with plane of IR)
Optic Canal Orbitoparietal oblique (Rhese) If a pt. cannot be done prone Will increase object magnification Greater exposure of lens of eye Can be done upright orrecument
Modified Waters • Before MRI is performed on any part of body, if even a suspicion patient has metal in eye, Waters must be taken • Particulary true in regions with lots of industry and manufacturing or welders and mechanics (at UCSF, a CT scan is done) • Why?
Modified Waters • Similar to Waters, but nose and chin touch IR • OML 50 deg angle. To IR • Gives better look into orbits-less foreshortening
R Modified WatersEvaluation Criteria Petrous ridges below orb. rims, but not below max. sinus Orbits symmetric, no rotation or tilt
L Lateral Orbit projection Similar to Lateral Sinus projection
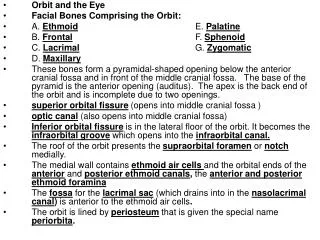
Parieto-orbital oblique • A- Superior orb.margin • B- lat. Orb Margin • C- optic foramin • D-Med.orb. Marg. • E- lesser wing of sphenoid • F- ethmoids • G- inferior orb. Marg. A B C D E F G
Optic Canal Parieto-orbital Evaluation Criterion • Optic foramina should lie in inferior lateral quadrant (4 o’clock or 8 o’clock) • Optic foramina should be seen enface at end of sphenoid ridge • Entire orbital rim must be shown, with close beam restriction R
Blowout Fx. of Orbit • Eyeball like small waterballoon • Fluid of eyeball will not compress • Eye ball capsule changes shape when hit • Force is transferred- floor of orbit is weakest
Tripod Fx. Of Zygoma • Blow to Zygoma (malar bone) breaks frontal, temporal and maxillary bones.-leaving Zygoma freely floating frontal temp max
Face is highly vascular- thus heals quickly This is both good and bad! • Good- fx. heals quickly • Bad- if cheekbone is depressed or out of place, heals - leaves face mis-shapen - will need to be rebroken, and reset
Name the 7 bones of Orbit • A- frontal • B- sphenoid • C- palatine • D- zygoma • E- maxillae • F- ethmoid • G- lacrimal
What projections? B A L R
What is the TMJ? • Where condyle of Mandible inserts into notch in Temporal bone
2 Types of Projections in TMJ Series Axiolateral AP Axial
8x10 LW Similar to Towne (which is 30 deg to OML, 2 ½ “ above glabella -how’s that different from 3” above Nasion?) Demonstrates condyles of mandible and mandibular fossa of temporal bone Collimate in! AP Axial TMJ’s
CR 35 deg. Caudad Midway between TMJs 3” above nasion First closed mouth, then open if not contraindicated AP Axial TMJ’s
No rotation of head Minimal superimposition of petrosa on condyle in closed mouth exam Open mouth may be performed if not contraindict. Condyle and temporomandibular articulation below pars petrose AP Axial TMJ’sEvaluation Criteria
TMJ Axiolateral projection • Place pt. head lateral position, effected side closest to IR (like lateral skull) • CR enters ½ “ ant., 2” superior to upside EAM • CR exits ½ anterior, 1” inferior to EAM affected side • CR angled 30 deg. Caudad 2” above EAM 1” below EAM
Temporomandibular ArticulationsAxiolateral projectionsSemi-prone Closed open
Temporomandibular ArticulationsAxiolateral projectionErect Open Closed
TMJ’s Axiolateral projections L L ? ?
All 4 projections are performed for TMJ Axiolateral Series Closed Open LEFT Closed Open RIGHT