Download
1 / 1
10 likes | 319 Views
Rare Case of Multicentric Castleman's Disease and Progressive Multifocal Leukoencephalopathy in a Severely Immunocompromised Patient. Noha Solieman 1 , Sherita N. Chapman 1 , Mohankumar Kurukumbi 1 ,Preema Mehta 2 ,Annapurni Jayam-Trouth

E N D
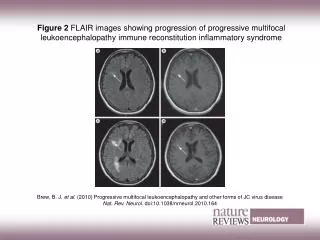
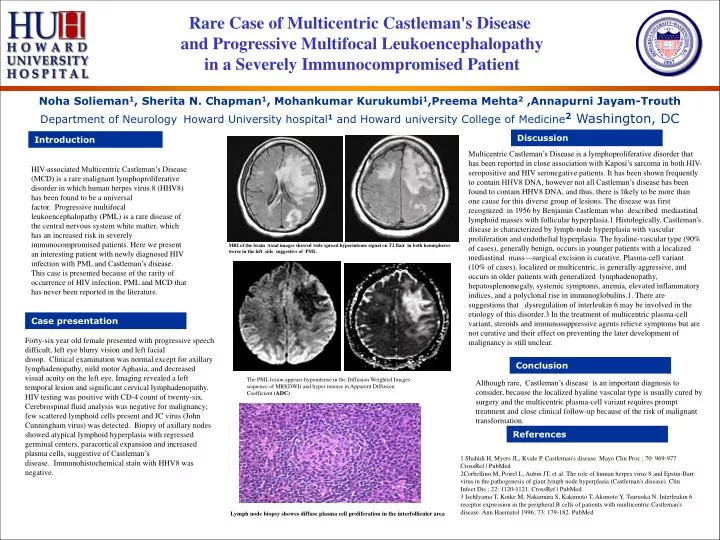
Rare Case of Multicentric Castleman's Disease and Progressive Multifocal Leukoencephalopathy in a Severely Immunocompromised Patient Noha Solieman1, Sherita N. Chapman1, Mohankumar Kurukumbi1,Preema Mehta2 ,Annapurni Jayam-Trouth Department of Neurology Howard University hospital1 and Howard university College of Medicine2 Washington, DC Discussion Introduction Multicentric Castleman’s Disease is a lymphoproliferative disorder that has been reported in close association with Kaposi’s sarcoma in both HIV-seropositive and HIV seronegative patients. It has been shown frequently to contain HHV8 DNA, however not all Castleman’s disease has been found to contain HHV8 DNA, and thus, there is likely to be more than one cause for this diverse group of lesions. The disease was first recognized in 1956 by Benjamin Castleman who described mediastinal lymphoid masses with follicular hyperplasia.1 Histologically, Castleman's disease is characterized by lymph-node hyperplasia with vascular proliferation and endothelial hyperplasia. The hyaline-vascular type (90% of cases), generally benign, occurs in younger patients with a localized mediastinal mass—surgical excision is curative. Plasma-cell variant (10% of cases), localized or multicentric, is generally aggressive, and occurs in older patients with generalized lymphadenopathy, hepatosplenomegaly, systemic symptoms, anemia, elevated inflammatory indices, and a polyclonal rise in immunoglobulins.1. There are suggestions that dysregulation of interleukin 6 may be involved in the etiology of this disorder.3 In the treatment of multicentric plasma-cell variant, steroids and immunosuppressive agents relieve symptoms but are not curative and their effect on preventing the later development of malignancy is still unclear. HIV-associated Multicentric Castleman’s Disease (MCD) is a rare malignant lymphoproliferative disorder in which human herpes virus 8 (HHV8) has been found to be a universal factor. Progressive multifocal leukoencephalopathy (PML) is a rare disease of the central nervous system white matter, which has an increased risk in severely immunocompromised patients. Here we present an interesting patient with newly diagnosed HIV infection with PML and Castleman’s disease. This case is presented because of the rarity of occurrence of HIV infection, PML and MCD that has never been reported in the literature. MRI of the brain Axial images showed wide spread hyperintense signal on T2 flair in both hemispheres worse in the left side suggestive of PML Case presentation Forty-six year old female presented with progressive speech difficult, left eye blurry vision and left facial droop. Clinical examination was normal except for axillary lymphadenopathy, mild motor Aphasia, and decreased visual acuity on the left eye. Imaging revealed a left temporal lesion and significant cervical lymphadenopathy. HIV testing was positive with CD-4 count of twenty-six. Cerebrospinal fluid analysis was negative for malignancy; few scattered lymphoid cells present and JC virus (John Cunningham virus) was detected. Biopsy of axillary nodes showed atypical lymphoid hyperplasia with regressed germinal centers, paracortical expansion and increased plasma cells, suggestive of Castleman’s disease. Immunohistochemical stain with HHV8 was negative. Conclusion The PML lesion appears hypointense in the Diffusion Weighted Images sequence of MRI(DWI) and hyper intense in Apparent Diffusion Coefficient (ADC) Although rare, Castleman’s disease is an important diagnosis to consider, because the localized hyaline vascular type is usually cured by surgery and the multicentric plasma-cell variant requires prompt treatment and close clinical follow-up because of the risk of malignant transformation. References 1 Shahidi H, Myers JL, Kvale P. Castleman's disease. Mayo Clin Proc ; 70: 969-977. CrossRef | PubMed 2Corbellino M, Poirel L, Aubin JT, et al. The role of human herpes virus 8 and Epstin-Barr virus in the pathogenesis of giant lymph node hyperplasia (Castleman's disease). Clin Infect Dis ; 22: 1120-1121. CrossRef | PubMed 3 IschIyama T, Koike M, Nakamura S, Kakimoto T, Akimoto Y, Tsuruoka N. Interleukin 6 receptor expression in the peripheral B cells of patients with muilticentric Castleman's disease. Ann Haematol 1996; 73: 179-182. PubMed Lymph node biopsy showes diffuse plasma cell proliferation in the interfolliculer area