Download

1 / 17
180 likes | 392 Views
Progressive Multifocal Leukoencephalopathy. July 31, 2007 Margo Smith, M.D. Department of Medicine Washington Hospital Center. Case 5.

E N D
Progressive Multifocal Leukoencephalopathy July 31, 2007 Margo Smith, M.D. Department of Medicine Washington Hospital Center
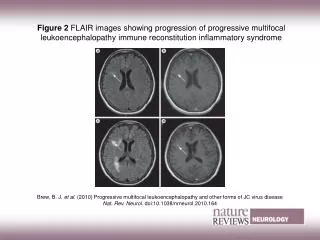
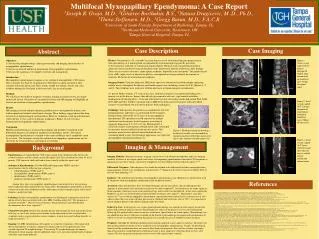
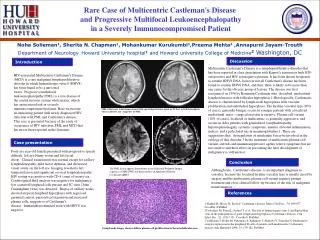
Case 5 • A 43 y o man with AIDS presents with a 4 week history of ataxia, progressive R hand weakness, and tremor. On exam he is ataxic and weak on the R when compared to his L side. He is afebrile, CD4 of 56/mm3 and a serum toxoplasma antibody was negative on his first visit to you and he does take TMP-SMX. You order a MRI and it shows a 2x4-cm lesion in the L cerebellar hemisphere on the T2-weighted images. There is no enhancement with gadolinium and no mass effect noted
Case 5 • The most likely diagnosis is? • A. Toxoplasmosis • B. Primary CNS lymphoma • C. Progressive multifocal leukoencephalopathy (PML) • D. Pyogenic brain abscess
Case 5 • The most likely diagnosis is? • A. Toxoplasmosis • B. Primary CNS lymphoma • C. Progressive multifocal leukoencephalopathy (PML) • D. Pyogenic brain abscess
Progressive Multifocal Leukoencephalopathy • Basics • JC virus, papovavirus (DNA) • 1958 first report • Cytolytic to oligodendrocytes – 5-HT2 receptor • Demylinating disease of brain • Optic nerve and spinal cord oligodendrocytes not affected
Progressive Multifocal Leukoencephalopathy • Asymmetric involvement • Brainstem – more common in AIDS • cerebellum • cerebral – 10:1 non-AIDS • Progresses to death rapidly
PML • Basics • Immunocompromised • AIDS • Leukemia • Symptoms • Cognitive, personality, motor weakness • Seizures
PML • Epidemiology • BK and SV40 related • ? Upper respiratory acquisition • Antibody prevalence increases with age • Latent virus reticuloendothelial system • No proof of CNS latency • 2 strains • Kidney • Brain
PML • HIV/AIDS • 2-5% • Viral DNA in ~ 55% peripheral lymphocytes • AIDS defining illness • CD4 < 100 • Dx • MRI – nonenhancing, no shift • CSF-PCR ~ 80% sensitive 90% specific
PML HIV/AIDS • Treatment • Highly active antiviral therapy • small studies • ~ 50% respond • ~ 50% progress • Immune reconstitution – BAD NEWS
PML • PML without HIV • T-cell immunodeficincy • Lymphoproliferative disorders • Chronic granulomatous diseases • Solid organ transplantation • Monoclonal antibody Rx • MS/Crohn’s Rx natalizumab 1:1000 • Hematologic malignancy prevalence ~ 0.07% • M:F = 3:2 • Pk age 60s
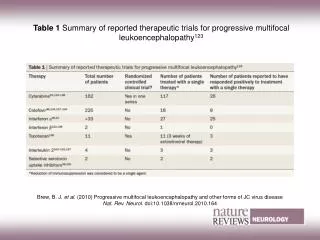
PML • Survival • AIDS weeks – months • Non-AIDS months – one year • Treatment Non-AIDS • Case reports • Interleukin-2 • Cytarabine • Cidofovir • 5-HT2 serotonin antagonizer – anti-depressant • Mitazapine = Remeron™
Dilemma Can one predict who is at risk to develop PML?
Progressive Multifocal Leukoencephalopathy • No pre-morbid serologic testing available • No pre-morbid CNS screen available • No pre-morbid imaging available • Not clear if there is an at risk subgroup • ~1/3 of healthy urine + JCV-DNA • Urine +JCV-DNA found more frequently immune suppressed • +JCV DNA mononuclear cells poor predictor
Progressive Multifocal Leukoencephalopathy • More questions and no clear answers • Does prior immune suppression increase risk? • If so, does the length of time increase risk? • Is there a role in monitoring antigen specific CD-8 cells? • Is a risk of 1:1000 reasonable?