Download
1 / 85
1.35k likes | 2.3k Views
IMPRESSION MATERIALS AND PROCEDURES IN REMOVABLE PARTIAL DENTURE. Presented by: Dr. Kamleshwar Singh BDS, MDS, ICMR-IF(Japan) Assistant Professor Department of Prosthodontics King George’s Medical University, Lucknow. INTRODUCTION Impression

E N D
IMPRESSION MATERIALSAND PROCEDURES IN REMOVABLE PARTIAL DENTURE Presented by: Dr. Kamleshwar Singh BDS, MDS, ICMR-IF(Japan) Assistant Professor Department of Prosthodontics King George’s Medical University, Lucknow
INTRODUCTION Impression • A negative likeness or copy in reverse of the surface of an object ; imprint of teeth and adjacent structures for use in dentistry. GPT – 8 Partial denture impression • A negative likeness of a part or all of a partially edentulous arch - GPT – 8
An impression of partially edentulous arch must record accurately the anatomic form of teeth and surrounding tissues. • Unless the cast upon which the prosthesis is to be constructed is an exact replica of mouth, the prosthesis can‘t be expected to fit properly and accurate cast can be obtained only from an accurate impression.
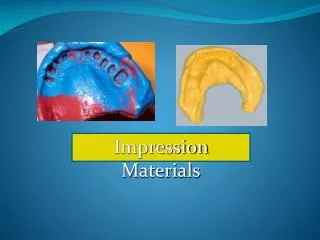
Impression trays A receptacle in to which suitable impression material is placed to make negative likeness OR A device that is used to carry, confine and control impression material while making an impression.
Impression trays can be classified broadly into stock trays and custom trays Stock trays for partially edentulous patients may be perforated to retain the impression material or they may be constructed with a rimlock for this purpose. Another type of stock tray designed for the reversible type of hydrocolloid is water cooled trays. It contains tubes through which water can be circulated for purpose of cooling the tray.
Modified stock tray (individual tray) Robert R Renner’s technique The stock tray can be modified with modeling composition and with wax to create an accurately fitting tray. This technique can be employed in class I and class II cases. Technique: Softened modeling compound is placed in the stock impression tray in such a way that it may capture the edentulous areas of mouth and include one or two teeth adjacent to the space.
Modified stock tray (individual tray) Robert R Renner’s technique The stock tray can be modified with modeling composition and with wax to create an accurately fitting tray. This technique can be employed in class I and class II cases. Technique: Softened modeling compound is placed in the stock impression tray in such a way that it may capture the edentulous areas of mouth and include one or two teeth adjacent to the space.
The tray is positioned in the mouth and compound is allowed to cool but it not permitted to harden completely, so that it is prevented from becoming hard when in contact with the adjacent teeth. When it is hardened sufficiently to contour it is removed from the mouth and thoroughly chilled.
The compound is trimmed so that it does not contact the adjacent teeth and surface of compound in the edentulous areas is scraped to a depth of 2 - 4 mm to provide space for a uniform layer of impression material. In maxillary impression the compound should cover the edentulous ridges and the palate and should accurately fit to post dam area.
Modification of the tray to make it adhesive If Impression material to be used is either alginate or agar, we can heat surface of compound with a flame. An alternate method Is to paint the surface of compound with a solvent such an chloroform to make it tacky and then to embed cotton fibers in it, the impression material will become enmeshed in cotton fiber. And if rubber base material is to be employed rubber adhesive is painted on the compound
Advantages over custom tray: 1. Impression can be accomplished in one appointment. 2. Can be used inpatient with tendency to gag. Advantages over conventional use of stock stray: Especially useful for mouth that is either exceptionally large or small or the one with anomalous contour which cannot be accurately fitted with conventional stock tray.
Disadvantages: STOCK TRAY a. The peripheral borders cannot be accurately recorded. b. Considerably more bulkier than a custom tray.
Custom impression trays: a. Peripheral borders can be precisely recorded in the impression b. Thickness of impression material can be controlled. This is important consideration when using rubber base type material, which should not exceed thickness of 2-4 mm because a section thicker than this is subject to distortion.
C. Well fitted tray will better support the impression in the palate, then avoiding even present danger of material slumping in vital areas. Custom trays are sometimes needed for mouths that are abnormally or of unusual configuration.
Factors that influence the selection of impression materials are: • Convenience of use • Time of manipulation and set • Cost • Need for special trays • Operator training and preference
Plaster Compound Waxes ZnO - Eugenol Polysulfide Silicones Polyether Non-elastic Impression Materials Agar (reversible) Aqueous Hydrocolloids Alginate (irreversible) Elastic Condensation Non-aqueous Elastomers Addition O’Brien Dental Materials & their Selection 1997
Reversible Hydrocolloid (Agar) • Indications • crown and bridge • high accuracy • Example • Slate Hydrocolloid (Van R)
Agar complex polysaccharide seaweed gelling agent Borax strength Potassium sulfate improves gypsum surface Water (85%) cool to 43 C agar hydrocolloid (hot) agar hydrocolloid (cold) (sol) (gel) heat to 100 C Composition O’Brien Dental Materials & their Selection 1997
Manipulation • Gel in tubes • syringe and tray material
Manipulation • 3 chamber conditioning unit • (1) liquefy at 100°C for 10 minutes • converts gel to sol • (2) store at 65°C • place in tray • (3) temper at 46°C for 3 minutes • seat tray • cool with water at 13°C for 3 minutes • converts sol to gel O’Brien Dental Materials & their Selection 1997
Advantages • Dimensionally accurate • Hydrophilic • displace moisture, blood, fluids • Inexpensive • after initial equipment • No custom tray or adhesives • Pleasant • No mixing required Phillip’s Science of Dental Materials 1996
Disadvantages • Initial expense • special equipment • Material prepared in advance • Tears easily • Dimensionally unstable • immediate pour • single cast • Difficult to disinfect Phillip’s Science of Dental Materials 1996
Irreversible Hydrocolloid (Alginate) • Most widely used impression material • Indications • study models • removable fixed partial dentures • framework • Examples • Jeltrate (Dentsply/Caulk) • Coe Alginate (GC America) Phillip’s Science of Dental Materials 1996
Sodium alginate salt of alginic acid mucous extraction of seaweed (algae) Calcium sulfate reactor Sodium phosphate retarder Filler Potassium fluoride improves gypsum surface 2 Na3PO4 + 3 CaSO4 Ca3(PO4)2 + 3 Na2SO4 H2O Na alginate + CaSO4 Ca alginate + Na2SO4 (powder) (gel) Composition O’Brien Dental Materials & their Selection 1997
Manipulation • Weigh powder • Powder added to water • rubber bowl • vacuum mixer • Mixed for 45 sec to 1 min • Place tray • Remove 2 to 3 minutes • after gelation (loss of tackiness) Caswell JADA 1986
Advantages • Inexpensive • Easy to use • Hydrophilic • displace moisture, blood, fluids • Stock trays Phillip’s Science of Dental Materials 1996
Disadvantages • Tears easily • Dimensionally unstable • immediate pour • single cast • Lower detail reproduction • unacceptable for fixed prosthodontics • High permanent deformation • Difficult to disinfect Phillip’s Science of Dental Materials 1996
RPD IMPRESSION Vs COMPLETE DENTURE The complete denture impression records the edentulous mucosa with underlying bone only, whereas partial denture impression records not only relative soft yielding tissues (the oral mucosa) as well as a hard unyielding substance (the remaining teeth).
Removable partial denture impression need to record the teeth that are irregular in contour as well as varying in their vertical relations to occlusal plane. The chosen impression material must be capable of recording the tissue contours as accurately as possible without distortion, which occurs as impression is withdrawn.
PRIMARY IMPRESSION Objectives: To obtain an impression of all the standing teeth and denture - supporting tissues of each jaw from which study casts may be prepared. The purpose of the study casts are:
To enable special trays and occlusion rims to be constructed if necessary. • To examine the occlusion in detail on an articulator. • By use of a surveyor, to plan the path of insertion of the proposed denture, arrive at a tentative design and plan any mouth preparation.
Checking Maxillary Tray For Correct Size Checking Mandibular Tray for Correct Size
Mixing Impression Material Alginate may be mixed by hand spatulation, mechanical spatulation, or mechanical spatulation under vacuum. The objective is to obtain a smooth, bubble- free mix of alginate. In hand spatulation a measured amount of distilled water at approximately 22 °C is placed in a rubber mixing bowl The pre-weighed alginate powder is sifted from its container into the water.
The mixing should begin slowly using a stiff, broad - bladed spatula.When the powder is thoroughly wet, the speed of the spatulation should be increased The spatula should crush the material against the sides of the bowl to ensure that the material is completely mixed. The spatulation should continue for a minimum of 45 seconds.
The strength of the gel can be reduced to 50 % if the mixing is not complete. Insufficient spatulation can result in failure of the ingredients to dissolve sufficiently. Then the chemical reaction of changing from sol to gel will not proceed uniformly throughout the mass of alginate. An incompletely spatulated mix will appear lumpy and granular and will have numerous areas of trapped air.
Complete spatulation will result in a smooth, creamy mixture. The mixing should be completed by wiping the alginate against the side of the bowl with the spatula to remove any trapped air. The most consistent method of making a smooth, bubble- free mix is mechanical spatulation under vacuum.
The pre-weighed powder is added to the pre-measured water in the mechanical mixing bowl .The powder is thoroughly incorporated into water by hand spatulation. The mix is then mechanically spatulated under 20 pounds of vacuum for 15 seconds.
Longer spatulation will result in a greatly reduced setting time of the alginate and could affect the strength of the gel.
Loading the Impression Tray Small increments of the impression material should be placed in the tray and forced under the rim lock. Placing too large a portion of alginate at one time increases the possibility of trapping air The tray should be filled to the level with the flanges of the tray. Overfilling should be avoided.
Making the Impression The mandibular impression is made first because it usually entails less patient discomfort patient confidence is increased when an impression has been successfully completed while holding the tray with the left hand the dentist uses the right hand to remove the gauze pads from the patient’s mouth.
The syringe is used to inject the impression material over the occlusal surface of the teeth and into the vestibular and alveolingual sulcus areas. The impression material will remain in place if the tissues are fairly dry. A tendency for the alginate to form a ball and not remain where placed indicates that the tissues are too moist and that voids are likely to be present in the impression.
There is not enough time to repack the mouth before gelation begins, so the impression procedure should be completed. The impression should be carefully inspected and if voids are present in critical areas, the impression procedure should be repeated. Packing the mouth with more or larger gauze pads and avoiding removal of the gauze until ready to apply the alginate will usually prevent this problem.
The layer of alginate applied with the syringe should be 3 to 4 mm thick; If it is too thin, the heat of the tissues of the oral cavity may cause the material to set before the tray is seated, resulting in a layered impression.
The fingers of the left hand that are retracting the right cheeks should depress the lower lip to provide good visibility. When the tray is correctly lined up over the teeth, the patient is asked to protrude the tongue. The tray is carefully seated so that its flanges are below the gingival margins of the teeth.
The tray should not be over seated because this could result in the cusps of the teeth contacting the tray, causing an inaccurate impression. Great care must be exercised in seating the tray if the patient has mandibular tori or other exostoses, or the making of this impression can be a very painful experience for the patient.
As the tray is being seated, the cheeks are pulled out to prevent the trapping of buccal tissues under the tray. The patient is asked to keep the tip of the tongue in contact with the upper surface of the tray during the gelation of the impression material.