Download
1 / 17
180 likes | 451 Views
Keeping Pre-ERSD Patients Pre-ERSD: Using the Health Belief Model. Nancy Roth, Ph.D. Chronic CKD. Major public health problem Estimated 20 million Americans have CKD Early detection and management can prevent disease progression

E N D
Keeping Pre-ERSD Patients Pre-ERSD: Using the Health Belief Model Nancy Roth, Ph.D.
Chronic CKD • Major public health problem • Estimated 20 million Americans have CKD • Early detection and management can prevent disease progression • Disease progression is associated with morbidity, mortality, costs and decline in QoL
Preventing ESRD • The biggest predictors of progression to ESRD are proteinuria, HTN and DM • There are significant challenges to working with patients to change their behaviors to reduce the likelihood of experiencing these complications • Several of these challenges are highlighted in the dimensions of the Health Belief Model
Challenges defined in Health Belief Model: • Perceived susceptibility—perception of personal vulnerability to a condition • Perceived severity—evaluation of medical/clinical consequences (death, disability, pain) and social consequences (work, family life, social relations) • Perceived benefits of action—perception of feasibility and efficacy of action • Perceived barriers—perceptions of action as expensive, dangerous, unpleasant, inconvenient, time-consuming
The Health Belief Model MODIFYING FACTORS INDIVIDUAL PERCEPTIONS LIKELIHOOD OF ACTION Demographic Variables (age, sex, race, ethnicity, etc) Sociopsychological variables Perceived benefits of preventative action Minus Perceived barriers to preventative action Perceived susceptibility to Disease “X” Perceived Seriousness (Severity) of Disease “X” Perceived Threat of Disease “X” Likelihood of Taking Recommended Preventative Health Action Cues to Action Mass Media Campaigns Advice from others Reminder postcards from physician or dentist Illness of family member or friend Newspaper or magazine article Health Education Quarterly (Spring 1984)
Applying the Health Belief Model to ESRD Prevention • By systematically looking at each dimension of the model, we can develop an approach to working with patients who are at risk for ESRD • We will use as a case a CKD patient with HTN and DM and focus on normalizing blood pressure and controlling sugar to prevent ESRD
Three Types of Patients YES NO MAYBE
Susceptibility • Patients vary in their perception of the extent to which they are personally vulnerable to disease • Helping patients to understand that they have a realistic probability of progressing is key
Case: CKD Patient with HTN and DM • How can we help patient to see the relationship between HTN, DM and ESRD? • Since HTN is “symptomless” what can we point to that will help the patient understand the impact of HTN on his/her health? • How can we help patients understand the severity of DM and its sequelae?
Severity • It is important for patients to understand that their disease has consequences that will affect their health and social life • There is some research that seems to contradict this • In some cases even when patients over-estimate their likelihood of progressing, they do not change their behaviors. • Increasing fear is not effective in motivating patients to change • We might conclude that it is necessary but not sufficient for patients to be aware of the impact on health and social life they face—and that the risks need to be presented in a way that raises awareness, but does not paralyze the patient
Case: CKD Patient who needs to control HTN and DM • What are the medical consequences of uncontrolled HTN and DM for a CKD patient? How can we help patient to understand them? • What are the social consequences of uncontrolled HTN and DM for a CKD patient? How can we help patient to understand them? • How can we do this in a way that motivates action rather than paralysis?
Benefits • To increase the likelihood of patients changing their behaviors, patients need to understand the benefits of action: efficacy and feasibility • It is difficult to demonstrate the efficacy of action when it is abstract: blood pressure means something to us as HCPs—but for patients, it is often just an abstract number • Decreasing that number is an abstract goal • And, patients perceive a number of barriers to behavior change (diet and exercise—and medication compliance) that make many of our recommendations seem impossible to implement
Case: CKD patient with HTN and DM • What are the benefits of controlling HTN and DM for a CKD patient? How can we explain this to the patient? • What would a patient need to do to control their HTN and DM? • How can we help a patient to find it feasible to implement those changes?
Barriers • Patients perceive a number of barriers that make behavior change difficult. • It is important to provide an atmosphere in which patients feel comfortable surfacing the issues and concerns about changing their behaviors • Once the concerns are on the table, joint problem solving can occur
Case: CKD patient with HTN and DM • What are some of the barriers to behavior change perceived by patients? • What might joint problem solving look like in your setting? • What would you need to do to make this feasible?
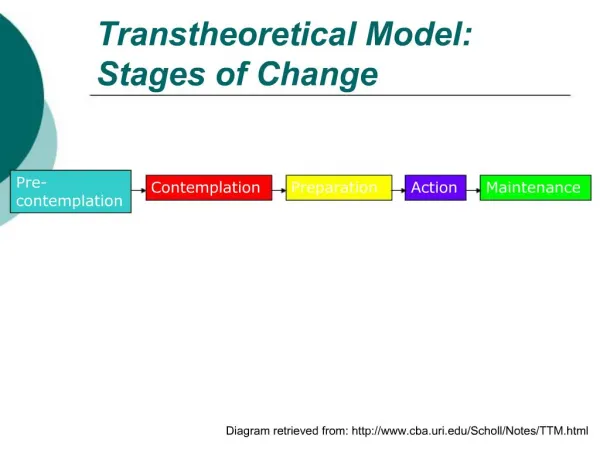
The Adherence Continuum Non-compliant pill irregularly pill regularly pill + behavior change
From Model to Practice • The Health Belief Model provides a useful framework for understanding some of the factors that influence the extent to which a patient will make behavior changes that can prevent disease progression. • We can use the model to help frame discussions with patients which lead to joint decision-making about how to work together to prevent disease progression.