Download
1 / 35
380 likes | 653 Views
RHINOSINUSITIS. DANIEL W. TODD, M.D. MIDWEST ENT. FORM (ANATOMY). FUNCTION (PHYSIOLOGY). FORM AND FUNCTION. ANATOMY (FORM). EXTERNAL NOSE (NASAL PYRAMID) NASAL CAVITY (SEPTUM & TURBINATES) PARANASAL SINUSES NASOPHARYNX. ANATOMY. NASAL PASSAGES BREATHING WARMING FILTERING

E N D
RHINOSINUSITIS DANIEL W. TODD, M.D. MIDWEST ENT
FORM (ANATOMY) FUNCTION (PHYSIOLOGY) FORM AND FUNCTION
ANATOMY (FORM) • EXTERNAL NOSE (NASAL PYRAMID) • NASAL CAVITY (SEPTUM & TURBINATES) • PARANASAL SINUSES • NASOPHARYNX
NASAL PASSAGES BREATHING WARMING FILTERING HUMIDIFYING OLFACTION (SENSE OF SMELL) RESISTANCE SINUSES LIGHTEN THE SKULL MUCOUS PRODUCTION HUMIDIFICATION PROTECT FROM FALCIAL TRAUMA PROTECT NASAL BAROTRAUMA VOCAL RESONANCE ENHANCE OLFACTION PHYSIOLOGY (FUNCTION)
Rhinosinusitis • Rhinosinusitis is the preferred terminology as you rarely have the sinusitis without the rhinitis. • The term is then further defined by the duration of the inflammation • ACUTE – LESS THAN 4 WEEKS • CHRONIC-MORE THAN 12 WEEKS
Rhinosinusitis • A GROUP OF DISORDERS CHARACTERIZED BY INFLAMMATION OF THE MUCOSA OF THE NOSE AND PARANASAL SINUSES • THERE IS NO CRITERIA BASED ON ETILOGY
RHINOSINUSITIS • REALLY AN IMFLAMMATORY DISORDER • NEED TO STOP THINKING OF IT AS SOLEY AN INFECTION
RHINOSINUSITIS---HOW DO YOU GET IT • INFLAMMATION---BLOCKING OF THE OSTIA—DIMINISHED PH---MUCOCILIARY DYSFUNCTION----STAGNATION OF SECRECTIONS---OVERGROWTH OF BACTERIA OR FUNGUS
RHINOSINUSITIS • INFLAMMATION CAUSED BY: VIRUS, ALLERGEN, IRRITANT, BACTERIA, FUNGUS • OMC: AREA OF RELATIVELY TIGHT ANATOMY
RHINOSINUSITIS • 60-90% OF SURGICAL PTS HAVE SIGNIFICANT ALLERGIES ON SKIN TESTING • THE MUCOSAL SPECIMENS ON ALL SURGICAL PTS DEMONSTRATE ALLERGIC INFLAMMATION
SUPERANTIGEN HYPOTHESIS • HIGH MOLECULAR WEIGHT PYROGENIC PROTEINS • ELICIT EXTREMELY POTENT STIMULATORY EFFECT ON T-LYMPHOCYTES
SUPERANTIGENS • BACTERIA (staph aureus, pseudomas, H influenza) • FUNGI (Molds, Candida, Bipolaris, Alternaria, Aspergillosis) • Allergens (Conventional and Bacterial antigens) • Irritants
SUMMARY • RHINOSINUSITIS IS AN INFLAMMATORY DISORDER OF THE NASAL PASSAGES AND PARANASAL SINUSES • IT’S ETIOLGY CAN BE EITHER INFECTIOUS (VIRAL, BACTERIAL, FUNGAL OR PARASITIC) OR NON-INFECTIOUS (ALLERGY, IRRITANT) • MAY HAVE ANATOMIC PREDISPOSITIONS
RHINOSINUSITIS • HOW DO YOU DIAGNOSE IT? • HOW DO YOU TREAT IT?
DIAGNOSIS • HISTORY • PHYSICAL • ENDOSCOPY • CT SCAN
MAJOR FACTORS FACIAL PAIN/PRESSURE NAO DISCHARGE HYPOSMIA PURULENCE FEVER MINOR FACTORS HEADACHE FEVER HALITOSIS FATIGUE DENTAL PAIN COUGH AURAL PAIN/FULLNESS DIAGNOSIS
MAXIMAL MEDICAL THERAPY • SALINE (SPRAY/IRRIGATIONS)—HYPERTONIC? • DECONGESTANTS (TOPICAL/SYSTEMIC) • MUCOLYTICS • STEROIDS (TOPICAL/SYSTEMIC) • ANTIHISTAMINES (TOPICAL/SYSTEMIC) • REFLUX THERAPY?
MAXIMAL MEDICAL • LEUKOTRIENE INHIBITORS • ANTIBIOTICS (TOPICAL/SYSTEMIC) • USUALLY START TREATMENT EMPIRICALLY---TREAT AT LEAST 1 WEEK PAST THE RESOLUTION OF SYMPTOMS (OFTEN 20 DAYS) • SINUNEB—IRRIGATIONS • CHRONIC---LOW DOSE CHRONIC BIAXIN
ALLERGY • THE NOSE IS THE TARGET ORGAN FOR AEROALLERGENS, IRRITANTS, AND DEBRIS. • TOPICAL THERAPIES AND NASAL RINSES ARE PARAMOUNT.
ALLERGY • ALLERGY TESTING AND TREATMENT IS NEVER A BAD IDEA PRIOR TO SURGERY • IDT IS THE MOST SENSITIVE AND SPECIFIC METHOD OF ALLERGY TESTING
SURGERY • THE CHRONIC INFLAMMATION FROM ALLERGIES AND INFECTIONS CAN LEAD TO ANATOMIC CHANGES • SINONASAL INFECTION IS A RELATIVE TERM • MOST MUCOSAL PROBLEMS ARE REVERSIBLE • SINUS SURGERY IS PLAN C
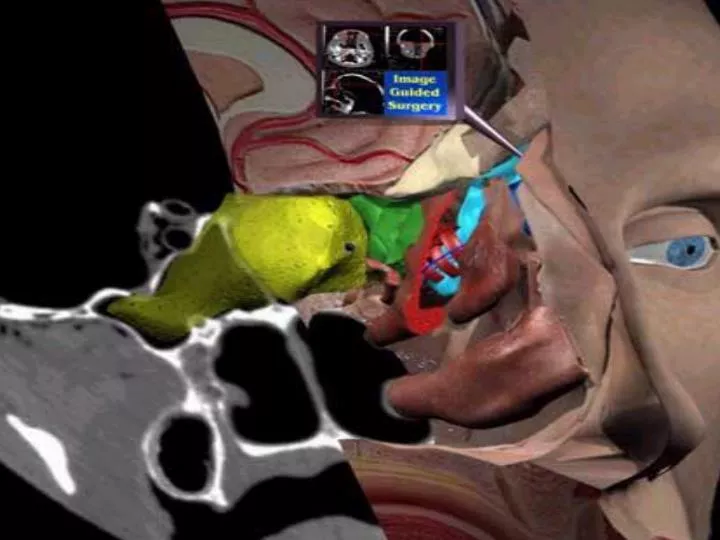
SINUS SURGERY • WE DO IT BETTER---UTILILIZE LASERS, ENDOSCOPES, TV MONITORS, MICRODEBIDERS, COMPUTER GUIDANCE SYSTEMS----STILL A DRAINAGE PROCEDURE
CONCEPTS • THE MOST HIGHLY TRAINED SINUS SURGEON IS A BOARD CERTIFIED OTOLARYNGOLOGIST (IN SINUS SURGERY THE MORE RECENTLY TRAINED THE BETTER) • THERE IS NO SUCH THING AS A SINUS SPECIALIST ALTHOUGH FELLOWSHIPS ARE EMERGING
CONCEPTS • SINUS SURGERY IS ALMOST NEVER AN EMERGENCY • PATIENTS WHO HAVE BEEN LURED IN BY DIRECT ADVERTISING SHOULD BE LESS LIKELY TO REQUIRE URGENT SURGERY THAN THE REFERRED PATIENT
NASAL CYCLE • LARGELY A FUNCTION OF THE INFERIOR TURBINATE • INFERIOR TURBINATE FULL OF VENOUS LAKES----SWELLS AND DECONGESTS • ALTERNATES SIDES---ON THE ORDER OF HOURS---PROBABLY ALLOWS THE NOSE TO CLEAN ITSELF