Download

1 / 42
480 likes | 813 Views
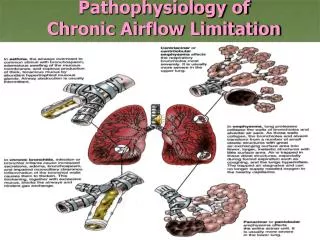
Upper Airways Research Laboratory Department of Otorhinolaryngology. New insights in the pathophysiology of chronic rhinosinusitis. PAUL VAN CAUWENBERGE, THIBAUT VAN ZELE, CLAUS BACHERT Ghent University, Belgium.

E N D
Upper Airways Research Laboratory Department of Otorhinolaryngology New insights in the pathophysiology of chronic rhinosinusitis PAUL VAN CAUWENBERGE, THIBAUT VAN ZELE, CLAUS BACHERT Ghent University, Belgium
Case reportMale, 46 yearsENT: nasal polyps since 12 years, 3 FESS surgeries, continuous use of topical GCSNo smell, nasal obstruction and PNDPneumo: moderate-severe asthma, AERD, inhalant and oral steroid use Your therapy?
CRS without NP CRS with NP EG2, X 100 H, X 100 CRS without and with NP Remodelling
TGF-beta in chronic sinus disease • Dual role: inflammation and remodelling • Immunmodulatory properties • Master switch in the induction of fibrosis • Three isoforms and three receptors described in humans prevalent form, until now most studied TGF-β1, TGF-β2, TGF-β3, TGF-β4, TGF-β5 • Three receptors: • TGFβrec1 • TGFβrec2 • TGFβrec3 or betaglycan humans
* TGF-beta 1 and 2 proteinin CRSs/wNP * * * * Van Bruaene et al, JACI 2009
Immunostaining Phospho-smad 2 Picrosirus red staining for collagen * * * * * * Van Bruaene et al, JACI 2009
CRSsNP CON CRSwNP A B C Picrosirius red 400× F D E Picrosirius red polarized light 400× Li X. et al, JACI 2010
CRS without NP CRS with NP EG2, X 100 H, X 100 CRS without and with NP TGFß1 low OEDEMA TGFß1 high FIBROSIS
Lack of T-regulatory cells in nasal polyps N. Van Bruaene, et al JACI, 2008
Inflammation in nasal polyposis: increased levels of inflammatory mediators IL-5 ECP P<0.001 P<0.001 P=0.016 P=0.086 ECP (µg/mL) IL-5 (pg/mL) Non-polyp NP I NP II NP III Non-polyp NP I NP II NP III Bachert et al. J Allergy Clin Immunol. 2001;107:607.
Treg and TH17: major revisions in the TH1/TH2 hypothesis of T cell differentiation Steinman, Nat Med, 2007
Different types of T effector cells orchestrate mucosal inflammation in chronic sinus disease Nan Zhang ; T Van Zele; Claudina Perez-Novo; N Van Bruaene; Gabriele Holtappels; Natalie DeRuyck; C Bachert. JACI 2008
Different types of T effector cells orchestrate mucosal inflammation in chronic sinus disease Nan Zhang ; T Van Zele; C Perez- Novo; N Van Bruaene; G Holtappels; N Deruyck; C Bachert. JACI 2008
Different types of T effector cells orchestrate mucosal inflammation in chronic sinus disease Nan Zhang ; T Van Zele; C Perez- Novo; N Van Bruaene; G Holtappels; N Deruyck; C Bachert. JACI 2008
70 nasal polyp tissue homogenates (Belgian patients) IL-5+ (58; 83%) IL-5- (12; 17%) 93 nasal polyp tissue homogenates (Chinese patients) IL-5+ (15; 16%) IL-5- (78; 84%) EOSINOPHILIC ?NEUTROPHILIC ?
CRS without NP CRS with NP EG2, X 100 H, X 100 CRS without and with NP Th2– Th17 Treg deficit Th1 Zhang N, Bachert C et al. JACI 2008
Zhang Nan, URL Ghent Staphylococcus aureus superantigens * 100 * 88 90 80 S. aureus colonization and IgE antibodies to S. aureus enterotoxin mix in mucosal tissue 80 * * 67 64 70 * S. aureus 54 60 colonization 50 SAE-IgE+ * 40 33 28 27 30 14 20 6 10 0 Controls CRS NP NP + NP + (n=9) (n=22) (n=53) asthma ASS
Nasal polyp tissue stained for S. aureus with PNA-FISH M-N. Corriveau, Zhang N Am J Rhinol, 2009
IL13 (pg/ml) IL4 (pg/ml) IL5 (pg/ml) Medians (error bars: 25-75 percentiles) Medians (error bars: 25-75 percentiles) Medians (error bars: 25-75 percentiles) 140 35 300 30 120 250 100 25 200 20 80 RPMI RPMI RPMI RPMI RPMI RPMI 150 15 60 SEB 0.5µg/ml SEB 0.5µg/ml SEB 0.5µg/ml SEB 0.5µg/ml SEB 0.5µg/ml SEB 0.5µg/ml 100 10 40 50 5 20 0 0 0 CO CO CO NP NP NP 24 hours stimulation ** ** ** ** ** ** ** ** * ** p<0.01 * p<0.05 (paired samples; Wilcoxon test/ Intergroup variability; Mann-Whitney U test) CO n=13 NP n=12 Patou J et al, JACI 2008
CD3 CD20 CD38 IgE SEA Follicle-like structures and lymphocyte accumulations in NP Gevaert P et al, Allergy 2005
T B S. aureus superantigens as disease modifiers Massive polyclonal lymphocyte activation Epithelial damage (barrier dysfunction) Hyper IgE Cytokines colonisation Multiclonal IgE Superantigens Eosinophil survival Fibroblast PGE2 prod. Chemokines Mast cell degranulation Review: Bachert C et al. Clin Allergy Immunol. 2007
Oral steroids in nasal polyps: a 3-month double blind, randomized, placebo-controlled trialDBPC in 32 patient with nasal polyps, 20days methylprednisolon(Day 1-5 32 mg, day 6-10 16 mg, day 11-20 8 mg) Thibaut Van Zele, Philippe Gevaert, Gabriele Holtappels, Achim Beule, Peter John Wormald, Susanne Mayr, Greet Hens, Peter Hellings, Fenna A Ebbens, Paul Van Cauwenberge, Claus Bachert
The future of treating persistent inflammation in polyp disease Antibiotics Anti-IgE IgE Anti-MMPs IL-5 Anti-IL-5 IKK2, SYK, iCRAC, PDE4 ECP Anti-CCR3 ?
Doxycycline reduces nasal polyp size in a DBRPC multicenter trial. 20 days doxycycline (100mg/d) * * Area under the curve Placebo: -145,4 Methylprednisolon: 530,6 P Gevaert, T Van Zele, G Holtappels, A Beule, PJ Wormald, S Mayr, G Hens, P Hellings, FA Ebbens, P Van Cauwenberge, C Bachert
* p<0,05 (Mann-Whitney) p<0,05 (paired Wilcoxon) Local anti-inflammatory effects of doxycyclin
The future of treating persistent inflammation in polyp disease Antibiotics Anti-IgE IgE Anti-MMPs IL-5 Anti-IL-5 IKK2, SYK, iCRAC, PDE4 ECP Anti-CCR3 ?
MEPO 750mg IV Placebo * Primary endpoints: polyp score, CT scan Dosing Follow up Study design Anti-IL-5 studyMepolizumab 2 x 750mg IV • Mepolizumab = a humanized anti-human IL-5 monoclonal antibody • 30 NP patients with recurrent bilateral nasal polyps after surgery or massive bilateral nasal polyps (Grade 3 or 4) 20 Subjects 30 Subjects Severe nasal polyps 10 Subjects Weeks 1 8 12 0 4 24 36 48 *
Endpoints Primary endpoint • Endoscopic Nasal polyp score 8 weeks post 1st dosing Secondary endpoints • CT scan assessment (blinded) • Symptom score • Peak nasal inspiratory flow • Local (nasal secretions) and systemic Inflammatory mediators • UPSIT smell test 1 0 3 2 4 Score 0 1 2 3 4
Endoscopic nasal polyp score improvement 13/20 12/20 10/20 intranasal steroids permitted * *
The future of treating persistent inflammation in polyp disease Antibiotics Anti-IgE IgE Anti-MMPs IL-5 Anti-IL-5 IKK2, SYK, iCRAC, PDE4 ECP Anti-CCR3 ?
PLACEBO SC OMALIZUMAB * Primary endpoint Dosing Follow up Objective and study design • To asses the therapeutic potential of • SC injections of anti-IgEOmalizumab (XOLAIR) • endoscopic score • symptom scores • CT scan • Two-arm, randomized, double blind, placebo controlled, trial 8 Subjects 24 Subjects Severe nasal polyps With asthma 16 Subjects 0 2 4 6 8 10 12 16 20 Weeks *
Inclusion criteria • At least 18 years of age • Bilateral severe nasal polyps with asthma • Recurrent nasal polyps after surgery OR • Grade 3 or 4 in both nares • Asthma defined on GINA guidelines (symptoms and lung function) • Serum IgE between 30 to 700 IU/ml • Good health, free of any clinically significant disease • Subjects with concurrent asthma must be maintained on no more than 1000 mcg/day BDP or the equivalent
Dosage and administration • Xolair 75 to 375mg is administered SC every 2 to 4 weeks (3 months) following official drug leaflet • Doses (mg) and dosing frequency are determined by total serum IgE level (IU/ml) measured at the start of treatment and body weight (kg) • Doses of more than 150mg are divided among more than 1 injection site • Injection every 4 weeks (4 injections) or 2 weeks (8 injections)
Improvement in symptomsOmalizumab (n=15) versus placebo (n=8)
Practical management of Nasal Polyposis • Nasal corticosteroids • GCS sprays: 2x/d, symptoms↓ • GCS drops: symptoms↓, surgery↓ • Oral corticoids: effective but fast recurrence • Antibiotics: • Antibiotic ointment • Long-term antibiotics: macrolides 500mg/d for 2m doxycycline 100 mg/d for 2m • Future: • Omalizumab (antiIgE; xolair) ? • Mepolizumab (anti-IL5) ?
Case reportMale, 46 years: nasal polyps, asthma, AERDNasal polyp score after 4 injections Omalizumab
Upper Airways Research Laboratory Department of Otorhinolaryngology Claus Bachert, MD, PhD Paul van Cauwenberge, MD PhD Philippe Gevaert, MD, PhD Nan Zhang, MD, PhD Thibaut Van Zele, MD, PhD Sofie Claeys, MD, PhD Claudina Novo-Perez, PhD Koen Van Crombruggen, PhD Olga Krysko, PhD Lara Derycke, PhD Joke Patou, MD Nicholas Van Bruaene, MD Wouter Huvenne, MD Peter Tomassen, MD Lien Devuyst, MD Takajuki Sejima, MD Marie-Noelle Corriveau, MD Gabi Holtappels Nathalie Deruyck Katrien Blomme