Download
1 / 37
370 likes | 734 Views
LAB 3: UPPER EXTREMITY: PART II – MUSCLE TESTING FOR SHOULDER, WRIST, AND HAND Group 4 Tyler Hyvarinen Aaron Ruberto Allison Pruys Kelly Heikkila Dr. Tony Bauer Kinesiology 3015 Lakehead University October 3, 2006. TENNIS ELBOW TEST (Lateral Epicondylitis).

E N D
LAB 3: UPPER EXTREMITY: PART II – MUSCLE TESTING FOR SHOULDER, WRIST, AND HAND Group 4 Tyler Hyvarinen Aaron Ruberto Allison Pruys Kelly Heikkila Dr. Tony Bauer Kinesiology 3015 Lakehead University October 3, 2006
TENNIS ELBOW TEST(Lateral Epicondylitis) The major muscles that attach to the lateral epicondyle are: extensor carpi radialis brevis, extensor carpi ulnaris, extensor digit minimi, extensor digitorum and the supinator Lateral epicondylitis is imflammation or irritation of these muscle attachments due to overuse or injury Steps to test for Tennis Elbow: Therapist stabilizes the patients forearm, applying slight pressure on the lateral epicondyle Patient makes a fist and extends the wrist The therapist will then apply pressure to the patients wrist, trying to gently force the wrist into flexion Observations should include if there is sudden, severe pain at the lateral epicondyle where the extensor muscles attach
MUSCLE TEST FOR WRIST FLEXION • Primary Flexors: • Flexor Carpi Radialis – Innervated by Median Nerve (C7) • Flexor Carpi Ulnaris – Innervated by Ulnar Nerve (C8,T1) • TESTING (While sitting or standing): • 1) Instruct thepatient to make a fist (this eliminates wrist flexion assistance from the finger flexors) • 2) Stabilize the wrist with your hand (as illustrated in the next slide) • 3) Tell patient to flex his or her closed hand at the wrist • 4) While wrist is in flexion place your hand over the patients flexed fist and offer resistance by trying to pull the patient’s wrist out of flexion
MUSCLE TEST FOR WRIST EXTENSION • Primary Extensors • Extensor Carpi Radialis Longus – Innervated by Radial Nerve (C6, C7) • Extensor Carpi Radialis Brevis – Innervated by Radial Nerve (C6, C7) • Extensor Carpi Ulnaris – Innervated by Radial Nerve (C7) • TESTING • *) Use the same methods as described in the muscle test for wrist flexion, but get patient to put closed fist in an extended position and offer resistance by trying to push the patient’s hand out of extension
MUSCLE TEST FOR WRIST SUPINATION • Primary Supinators • Biceps – Innervated by Musculocutaneous Nerve (C5,C6) • Supinator – Innervated by Radial Nerve (C6) • Secondary Supinator • Brachioradialis • TESTING • 1) Position yourself in front of the patient with your hand supporting the patient’s elbow at the side (the support will aid in eliminating shoulder abduction and external rotation of the forearm in place of forearm supination) • 2) Place the thenar eminence of your hand on the dorsal surface of the patient’s radius (distal) • 3) Wrap your finger around the ulna (medially) • 4) Tell patient to begin supination from a position of pronation • 5) As the patient further progresses the supination of his/her forearm, increase your resistance against the radius – this will determine the maximum resistance the patient can overcome
MUSCLE TEST FOR WRIST PRONATION • Primary Pronators • Pronator Teres – Innervated by Median Nerve (C6) • Pronator Quadratus – Innervated by Anterior Interosseous Branch of Median Nerve (C8,T1) • Secondary Pronator • Flexor Carpi Radialis • TESTING • *)Use the same procedures as described in the muscle test for wrist supination, but adjust your resisting hand so that the thenar eminence presses against the frontal-distal surface of the radius. Get the patient to begin forearm pronation from a position of supination. Offer increased resistance as patient increases pronation of his/her forearm.
MUSCLE TEST FOR FINGER EXTENSION • Primary Extensors: • Extensor Digitorum Communis – Innervated by Radial Nerve (C7) • Extensor Indicis – Innervated by Radial Nerve (C7) • Extensor Digiti Minimi – Innervated by Radial Nerve (C7) • TESTING • 1)Stabilize the patient’s wrist in a neutral position • 2)Get patient to extend his/her metacarpophalangeal joints, while flexing the proximal interphalangeal joints (this prevents the aid the intrinsic muscles of the hand may make in place of the long finger extensors) • 3)Place your hand on the dorsum of the proximal pahalanges and try to force them into flexion
MUSCLE TEST FOR FINGER FLEXION • Primary DIJ Flexor • Flexor Digitorum Profundus – Innervated by Ulnar Nerve and Anterior Interosseous branch of Median Nerve (C8,T1) • Primarty PIJ Flexor • Flexor Digitorum Superficialis – Innervated by Median Nerve (C7,C8,T1) • Flexors of Metacarpophalangeal Joint • Lumbricals – Medial 2 – Innervated by Ulnar Nerve (C8) • Lumbricals – Lateral 2 – Innervated by Median Nerve (C7) • TESTING • 1)Have patient flex his/her fingers st all phalangeal joints • 2)Curl and lock your fingers into the patients’ and try to pull his/her finger out of flexion • 3)All joints should remain flexed – Make note of those specific joints that fail to hold against your resistance
MUSCLE TEST FOR FINGER ABDUCTION • Primary Abductors • Dorsal Interossi – Innervated by Ulnar Nerve (C8,T1) • Abductor Digiti Minimi – Innervated by Ulnar Nerve (C8,T1) • TESTING • 1)Have your patient abduct his or her extended fingers away from the axial midline of the hand • 2)Try to force each pair of the patient’s fingers together • Pinch index finger to the middle, ring, and little fingers • Pinch the middle finger to the ring and little fingers • Pinch the ring finger to the little finger
MUSCLE TEST FOR FINGER ADDUCTION • Primary Adductors • Palmar Interossei – Innervated by Ulnar Nerve (C8,T1) • TESTING • 1)Have your patient keep his/her fingers extended together • 2)See muscle test for finger abduction – instead of pinching the fingers together, pull the same pairs of fingers apart • Alternate Method • 1)Place a piece of paper between two of the patient’s fingers • 2)Get the patient to hold the piece of paper between his fingers while you try to pull it out from between ON ALL TESTS: The strength of the patient’s grasp on one hand should be compared to the opposite
THUMB EXTENSION Muscles primarily involved in thumb extension include the extensor pollicis brevis (metacarpophalangeal joint) and extensor pollicis longus (interphalangeal joint), which are both innervated by radial nerve, C7 Steps for thumb extension muscle testing: Patient extends thumb Therapist will press upon the distal phalanx which will push the thumb into flexion Observations should include if either joint of the thumb flex with little pressure applied, indicating muscle weakness Weakness will be apparent if the patient uses thumb abductors in order to perform the extension
THUMB FLEXION • Muscles primarily involved in thumb flexion include the flexor pollicis brevis (metacapophalangeal joint) which is innervated medially by the ulnar nerve (C8) and laterally by the median nerve (C6, C7) and also the flexor pollicis longus (metacapophalangeal joint) which is innervated by the median nerve (C8, T1) • Steps for testing thumb flexion: • Patient flexes thumb toward his hypothenar eminence • Therapist will now hook his thumb into patients and try to pull thumb out of flexion • Observe if thumb is easily pulled out of flexion, indicating muscle weakness or malfunction
THUMB ABDUCTION(Palmar abduction) • Primary muscles involved in thumb abduction are the abductor pollicis brevis which is innervated by the median nerve (C6, C7) and the abductor pollicis longus which is innervated by the radial nerve (C7) • Steps for thumb abduction: • Therapist will stabilize patient’s metacarpals along the ulnar border with one hand and hold the patient’s thumb with the other hand • Patient will attempt to abduct the thumb fully as the therapist attempts to push thumb toward the palm • Note that if the patient attempts to substitute the movement with thumb extensor muscles, the abductor pollicis brevis and longus may be weak or damaged
THUMB ADDUCTION • The primary muscles for thumb adduction is the adductor pollicis (obliquus and transverus) which is innervated by the ulnar nerve (C8) • Steps for testing thumb adduction: • Therapist will stabilize patient’s metacarpals along the ulnar border with one hand and hold the patient’s thumb with the other hand • Patient will attempt to adduct the thumb while the therapist applies gradual resistance • Observations should include the maximum resistance the patient can overcome while adducting
PINCH MECHANISM(Thumb and index fingers) • The main muscles responsible for creating an “O” shape between the thumb and index fingers are the long flexors and extensors, which stabilize the interphalangeal, metacarpophalangeal and carpometacarpal joints. • Also included in the pinching motion are the lumbricals and interossus membrane • Steps for testing the pinch mechanism: • Patient touches the tips of their thumb and index finger together • Therapist will curl their index finger around the union of the patients finger and thumb and attempt to pull them apart • Observations should include the strength of the pull required – if there is injury in the muscles, the “O” shape will collapse with little force
OPPOSITION OF THUMB AND LITTLE FINGER • The primary muscles involved in opposition are the opponens pollicis, which is innervated by the median nerve (C6, C7) and the opponens digiti minimi, which has innervation from the ulnar nerve (C8) • Steps for testing opposition: • Patient will touch the tips of his little finger and thumb together • Therapist will grasp the thenar eminence with one hand and the hypothenar eminence with the other hand, palpating for the underlying metacarpals • Therapist will then attempt to separate the tips of the patients fingers by pushing the metacapals away from each other
TESTING MUSCLE SENSATIONWrist & Hand • Sensation in the wrist and hand should be tested in two ways: • Testing each Neurologic Level involved in the hand • Testing the major Peripheral Nerves that innervate the hand
PROCEDURES AND EQUIPMENT FOR TESTING HAND NEUROLOGIC LEVELS (DERMATOMES) & PERIPHERAL NERVES • Muscle sensation is evaluated using a Wartenberg Pinwheel as pictured. Tests of sensitivity of peripheral nerves or neurologic levels may also be done using a cotton ball, paperclip, pads of fingers or fingernails. • (http://www.sagewoodwellness.com/Doc0004.htm) • The pins on the Wartenberg Pinwheel may also be used as a single point mechanism for peripheral nerve testing. • TESTING HAND NEUROLOGIC LEVELS (Dermatomes): • Ask patient to sit or lie down in a comfortable position. • Make sure the patient is aware that he/she should not feel any pain or discomfort. • Using the Wartenberg Pinwheel, roll it gently over the specified dermatome in the hand. • Have the patient provide you with feedback regarding sensation. • TESTING PERIPHERAL NERVES: • Ask the patient to first sit or lie down in a comfortable postion. • Make sure the patient is aware that at no point in time should they feel any discomfort or pain. • Gently apply pressure with the point tool (as listed above) to the area specified for particular nerve sensation. Table 2 • Have the patient give you feedback on the type of sensation present. The patient should have feeling in the area tested, however sensation should not be excessive Note: Dermatomes are always tested before Specific Peripheral Nerves
TESTING HAND NEUROLOGIC LEVELS • The sensation in the hand is provided by 3 neurologic levels found in the cervical spine: • C6 • C7 • C8
DERMATOME FOR NERVE ROOT C6 • Spinal nerve root C6 provides sensation to the lateral forearm, innervating most of the forearm extensors. • Distally C6 fibers form the Median Nerve. • To test sensation of the C6 nerve root, roll the Wernberg Pinwheel gently over the lateral aspect of the palm to the index (2nd digit) finger and over the thumb. • The muscles innervated by C6 fibers are: Serratus anterior, Deltoid, Infraspinatus, Teres minor, Supraspinatus, Teres major, Pectoralis major, Latissimus dorsi, Biceps, Brachialis, Brachioradialis, Supinator, Pronator teres, Flexor carpi radialis, Extensor carpi radialis, & Extensor digitorum communis.
DERMATOME FOR NERVE ROOT C7 • Spinal nerve root C7 provides sensation to the proximal forearm and hand muscles, mainly the wrist flexors and finger extensors. • Distally C7 fibers form the median and radial nerves. • To test sensation of the C7 nerve root, gently roll the pinwheel over the dorsal and ventral (palm) hand over the 3rd and 4th digits. • The muscles innervated by C7 fibers are: Latissimus dorsi, Pectoralis major, Triceps, Pronator teres, Flexor carpi radialis, Extensor carpi radialis, Palmaris longus, Extensor digitorum communis, Extensor indicis proprius, flexor digitorum superficialis, Abductor policis longus, Extensor policis brevis, Extenosr policis longus, Extensor carpi ulnaris, and Flexor carpi ulnaris.
DERMATOME FOR NERVE ROOT C8 • Spinal nerve root C8 provides sensation to both the proximal and distal muscles. Distally, C8 fibers innervate the finger flexors and form the median, ulnar and radial nerves. • To test sensation of the C8 nerve root in the hand, gently roll the pinwheel over the medial aspect of the dorsal and ventral hand – up the 4th and 5th digits. • The muscles innervated by C8 fibers are: Latissimus dorsi, Pectoralis major, Triceps, Palmaris longus, Flexor digitorum superficialis, Flexor policis longus, Abductor policis longus, Extensor policis brevis, Extensor policis longus, Extensor carpi ulnaris, Flexor carpi ulnaris, Flexor digitorum profundus, Lumbricals, and Interossei.
TESTING PERIPHERAL NERVE SENSATION • The hand is supplied by 3 major peripheral nerves: • Radial Nerve • Median Nerve • Ulnar Nerve
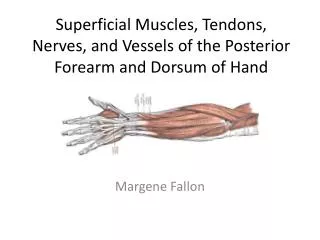
THE RADIAL NERVE TEST • The radial nerve supplies the dorsal surface of the hand on the radial side of the third metacarpal, as well as the dorsal surfaces of the thumb, index and middle fingers. • The area most fully innervated by the radial nerve, and used in testing radial nerve sensation, is the web space on the dorsal surface of the hand, found between the thumb and index fingers. • The muscles innervated by the radial nerve are the: triceps, brachialis, brachioradialis, anconeus, supinator, extensor carpi radialis longus, extensor carpi radialis brevis, extensor carpi ulnaris, extensor digitorum communis, extensor digiti minimi, abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, & the extensor indicis. http://classes.kumc.edu/sah/resources/handkines/nerves/radial.htm
THE MEDIAN NERVE TEST • The median nerve innervates the radial side of the palm. The ventral surfaces of the thumb, index and middle fingers are also supplied by the median nerve. • Strongest sensation from the median nerve can be found on the ventral/palmar skin of the tip of the index finger (2nd digit). This is where median nerve sensation is tested. • The muscles innervated by the median nerve are the:pronator teres, palmaris longus, flexor carpi radialis, flexor digitorum superficialis, flexor digitorum profundus (lateral portion), pronator quadratus, flexor pollicis longus, abductor pollicis brevis, opponens pollicis, & the flexor pollicis brevis. http://classes.kumc.edu/sah/resources/handkines/nerves/median.htm
THE ULNAR NERVE TEST • The ulnar nerve innervates both the dorsal and ventral/palmar surfaces of the ulnar side of the hand. It also supplies the same surfaces on the 4th and 5th digits. • Sensation is strongest on the lateral tip of the 5th digit. This is were sensation testing occurs. • The muscles innervated by the ulnar nerve are the: Flexor carpi ulnaris, Flexor digitorum profundus, Palmaris brevis, Adductor pollicis, Flexor pollicis longus, Abductor digiti minimi, Opponens digiti minimi, & the Flexor digiti minimi. http://classes.kumc.edu/sah/resources/handkines/nerves/ulnar.htm
Muscles Involved Lumbricles at the Metacarppohalangeal joint Flexor digitorum superficialis at the Proximal Interphangeal joint Flexor digitorum profundas at the Distal Interphangeal joint Joints Involved Metacarpo-phalangeal Joints Proximal Interphalangeal Joints Distal Interphalangeal Joints Nerve Supply Lumbricales – Lateral 2 by Median Nerve, Medial 2 by Ulnar Nerve Flexor Digitorum Superficialis – Median Nerve Flexor Digitorum Profundus – Ulnar Nerve FINGER FLEXION(Special Tests)
FLEXOR DIGITORUM SUPERFICIALIS TEST • The Flexor Digitorum Superficialis tendon is the only functioning tendon at the proximal interphalangeal joint • The distal interphalangeal joint powered by the flexor digitorum profundus has no power of flexion when the other fingers are held in extension, and the finger tip is loose and beyond the patient’s control. • Steps for Testing • Hold the patient’s fingers in extension except for the finger being tested. This isolates the flexor digitorum superficialis. • Instruct the patient to flex the finger being tested at the proximal interphalangeal joint. • Note whether or not the patient is able to flex their finger. If they can flex their finger, the FDS tendon is in tact. If they cannot flex their finger at the specified joint, the tendon is either cut or absent.
FLEXOR DIGITORUM PROFUNDUS TEST Note that the flexor digitorum profundus tendons work only in unison, therefore if the patient is unable to individually flex at any given interphalangeal joint Steps for test: Therapist will isolate the distal interphalangeal joint by stabilizing the metacarpphalangeal and interphalangeal joints in extension Have the patient flex his finger at the distal interphalangeal joint If the patient cannot flex his finger at the distal interphalangeal joint, the tendon may be cut or the muscle denervated
RETINACULAR TEST • This tests function is to determine whether flexion limitations at the distal interphalangeal joints are due to tightness of the retinacular ligaments or to joint capsule contractures Steps for retinacular test: • Therapist will hold the proximal interphalangeal joint in a neutral position and try to move the distal interphalangeal joint into flexion • If the joint does not flex, there are two conclusions to be made – there is either joint capsule contraction or retinacular tightness • To test if it is retinacular tightness, the therapist will flex the proximal interphalangeal joint slightly to relax the retinaculum. If the proximal interphalangeal joint flexes, the patient is positive for retinacular tightness • If the proximal interphalangeal joint does not flex then the interphalangeal joint capsule is probably contracted
ALLEN TEST • Evaluates • This test makes its possible to see I the radial and ulnar nerves are supplying the hand. • TESTING • Instruct the patient to open and close their fist quickly several times, then to close their fist tightly so that the venous blood is forced out of the palm. • Place your thumb over the radial artery and your index and middle fingers over the ulnar artery, and press them against the underling bone to occlude them. • With the vessels still occluded, instruct the patient to open their hand. The palm of the hand should be pale. • Then release one of the arteries at the wrist, while maintaining pressure on the other one. • Normally blood will return to the hand immediately. If it does not react of blood comes back slowly, then the released artery is partially or completely occluded. • The opposite artery should also be checked the same way.
Allen test for fingers • Follow the same procedure for the Allen test, except.. • With the hand still in a fist lace your index and middle finger on the sides of the finger being tested, pressing them o the bone to occlude the digital arteries. • When the patient opens their hand the test finger should be pale. • The blood normally returns to the finger when pressure is released. If it does not the flow of the digital arteries is in question.
BUNNEL-LITTLER TEST • Evaluates: • Tightness of the intrinsic muscles of the hand • Whether flexion limitation in the proximal interphalangeal joint is due to tightness of intrinsic muscles of the hand or to joint capsule contractures (prevents the finger from curling into the palm) • TESTING • 1) Hold the patient’s metacarpophalangeal joint in slight (few degrees) extension (fig.112) • 2) Try to move the proximal interphalangeal joint into flexion (fig.113) • 3) If proximal interphalangeal joint can be flexed, the intrinsics are not tight (not limiting flexion) • 4) If proximal interphalangeal joint can’t be flexed, the intrinsics are tight or there are Joint Capsule Contractures • Distinguishing between intrinsic muscle tightness and Joint Capsule Contractures • Let the patient’s finger (one being tested) flex a few degrees at the metacarpophalangeal joint (this relaxes the intrinsic muscles and moves the proximal interphalangeal joint into flexion) • If the joint is capable of full flexion – Intrinsics are most likely tight (fig.114) • If the joint does not flex – Limitation is probably due to proximal interphalangeal joint capsule contractures (fig.115)
REFERENCES All material unless otherwise noted retrieved from: Hoppenfield. S. Physical Examination of Spine and Extremities. Appleton Croft. 1972.