Download
1 / 17
170 likes | 277 Views
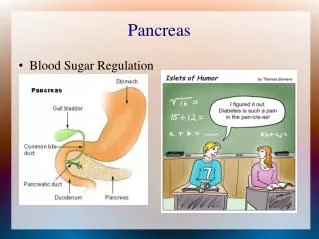
Pancreas Review. I am made in K cells and travel to the pancreass after meals to increase insulin release. GIP I target the biliopancreatic system after meals and increase pancreatic bicarb secretion and also the delivy of bile. CCK

E N D
I am made in K cells and travel to the pancreass after meals to increase insulin release. GIP I target the biliopancreatic system after meals and increase pancreatic bicarb secretion and also the delivy of bile. CCK I am mostly produced in the pancreas, and target the liver to increase glycogenolysis and gluconeogenesis. I am inhibited by somatostatin. I also go to fat and increase lipolysis and ketogenesis. Glucagon Similar to CCK, I increase panc and bile secretion. I can be used to help diagnose hypergastrinemia. Secretin Stimulated by presence of CCK, I inhibit pancreatic secretion, and GB contraction, and slow down the foregut in the post-prandial state Panc. PP Bonus: How is PPP used clinically? Tumor marker for APUDoma’s Stimulated by intraluminal fat, I also slow down the foregut in the post-prandial state Peptide YY
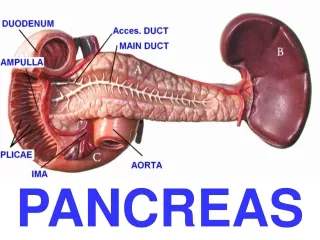
What is the name of the main pancreatic duct The Duct of Wirsung Mindless fact: Wirsung was murdered in Padua in 1643 over a fight about who really discovered the duct. Dr. Bartholin was also a co-discoverer. What is the name of the small pancreatic duct Duct of Santorini Santorini was a Venetian anatomist and his star pupil was Vater. What did Vater name? Where is the Supreme Artery of Kirk Dorsal Pancreatic artery
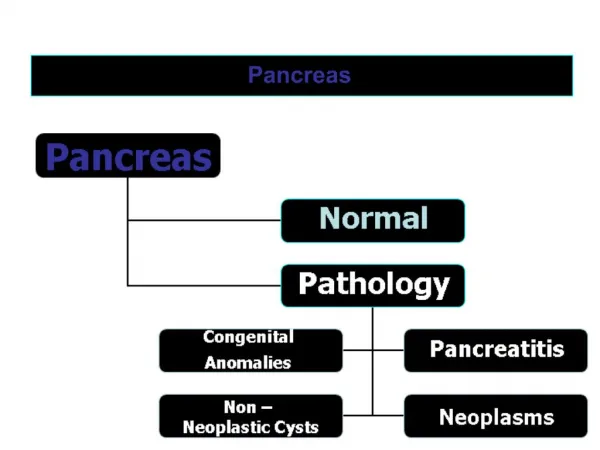
Which pancreatic bud is connected to the bile duct Ventral Which bud migrates posteriorly and left to fuse with the other Ventral migrates towards dorsal Which duct comes from the ventral bud Wirsung What does the ventral bud become Uncinate and inferior head The dorsal bud has the duct of wirsung and makes up the sup. Head, body, and tail
Which bud abnomally fuses and causes an annular pancreas? The ventral bud migrates ant and post but fails to fuse How does it present and what is common pre-existing co-morbidity Bowel obstruction in newborn period , Down’s syndrome. What is the treatment Duodeno-duodenostomy What condition is caused by failure of ducts to fuse Pancreatic divisum Who do you treat and what is treatment Recurrent attacks, ERCP/sphincterotomy/papillotomy, lap chole.
Which common meds are associated with pancreatitis Proven: Azathioprine, Lasix, depakote, thiazides, tetracycline, sulfonamide, H2 blockers Suspected: steroids, Tacrolimus, flagyl, 6-mp What metabolic causes can cause pancreatitis Hypertriglycidemia, and hypercalcemia What surgical diseases may cause pancreatitis Perforated peptic ulcer, crohn’s of duodenum
Which enzymes are responsible for Acute pancreatitis Trypsin Pancreatic necrosis (in the presence of bile) Phospholiapse A Intrapancreatic hemorrhage Elastase Bonus: How does PLA2 affect lungs during pancreatitis By digesting pulmonary surfactant and causing ARDS
What signs are seen on a flat-plate for acute pancreatitis Sentinel loops, colon cut-off, dilated duodenum What is a sentinel loop Adynamic dilated loop of SB with small focal area of inflammation related to panc. Associated ileus. What signs are seen on a flat-plate for chronic pancreatitis Calcifications On CT? Dilated panc. Duct, calcifications, parenchymal atrophy On ERCP Chain of lakes
What are the early ranson’s criteria Age >55 WBC >18k Glucose>220 LDH>40 AST>250 What are the late criteria? HCT drop >10 + fluid sequ by 4L BUN up by 5 from baseline Ca<8 BD>5 pO2 <55
Which of the following are indications for necrosectomy? >50% pancreatic necrosis by CT Bile duct stricture Refractory Shock for >3 days Infected necrosis What % of people with GB pancreatitis will recur within 8 weeks if GB not removed 33%
What are the absolute indications for surgery in chronic pancreatitis? None Relative indications? Refractory disabling pain GI or biliary obstruction Recurrent acute exacerbations Splenic V thrombosis with portal HTN r/o malignancy
What % of patients with acute pancreatitis will get a pseudocyst? 20% What % of patients with chronic pancreatitis will get a pseudocyst? 20-40% What % of patients with acute pancreatitis will get a persistant pseudocyst? <5% What is most common cause for children to get pseudocyst Trauma
What % of periampullary tumors come from: The pancreas? 40-60%. CBD? 10% Duodenum? 10% Ampulla itself? 20-40% What tumor marker is the most useful CA 19-9 has the highest sens and spec.
Which genetic syndromes and genes assoc. with panc ca BRCA 2, HNPCC, Peutz-Jeghers, MEN1, p-53 What is the most common benign neoplasm in the pancreas Cystadenoma What is the most common cystic lesion in the pancreas Pseudocyst Courvoisier lived in Switzerland in 1880’s and fought in Franco-Prussian (7-years war). Did internships with Lister and Bilroth
What rash do patients with glucagonoma get Nec Mig Ery. Also anemia, glossitis, and weight loss (rem: all malignant) What do patients with VIPomas get WDHA (rem: 50% malignant) What do patients with somatistatinomas get Gallstones, DM, and steatorrhea (rem: all malignant) What will the question mention in gastrinoma? H. Pylori negative. (1/2 malig), never malign when in MEN 1 (10% of time) Bonus: 2nd most common location of gastrinoma following pancreas Duodenum. (submucosal) in triangle
Who am I? Sunburst pattern on CT, rarely malignant Serous cystadenoma ( Sunny and not Serious) I am frequently malignant and have peripheral calcifications Mucinous (M Malig) I am premalignant and require excision with clear margins “fishmouth” duct with mucus pathogen. IPMT