Download
1 / 67
810 likes | 1.28k Views
25 May 2012 Dept. of Diagnostic Radiology UFS M. Pieters. Imaging Anatomy of the Wrist. The wrist. Osseous structures Ligaments Tendons Neurovascular structures. Anatomical variants. Osseous structures. Trapezoid. Hook of Hamate. Trapezium. Hamate. Capitate. Pisiform. Triquetrum.

E N D
25 May 2012 Dept. of Diagnostic Radiology UFS M. Pieters Imaging Anatomy of the Wrist
The wrist • Osseous structures • Ligaments • Tendons • Neurovascular structures Anatomical variants
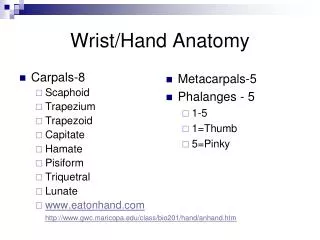
Osseous structures Trapezoid Hook of Hamate Trapezium Hamate Capitate Pisiform Triquetrum Scaphoid Lunate Radius Ulna
Osseous structures Lateral radiograph obtained in zero-rotation position. Note the position of the pisiform overlying the mid waist of the scaphoid indicates a properly positioned lateral
Carpal bone ossification The capitate ossifies first and the pisiform last But the order and timing of the ossification of the other bones is variable Excluding the pisiform, they ossify in a clockwise direction from capitate to trapezoid as follows: Capitate Hamate Triquetral at 3 years Lunate bone at 5 years Scaphoid, trapezium and trapezoid at 6 years The pisiform ossifies at 11 years of age at 4 months
The midcarpal and radiocarpal joint are seperated by interosseous ligaments No communication Complex palmar and dorsal ligaments provide support Arthrogaphy – ideally conducted in 3 stages Compartments, joints and ligaments
Osseous structures - joints • Distal (inferior) radioulnar joint: Pivot joint; ROM: Distal radius rotates around distal ulna • Radiocarpal joint: Ellipsoid joint created by proximal carpal row articulating with distal radius & ulna ROM: Flexion, extension, abduction, adduction, circumduction, no rotation
Osseous structures - joints • Pisotriquetral: Gliding joint created by pisiform and triquetrum; Discretely separate from radiocarpal joint in 10-25%; ROM: Minimal • Midcarpal: Gliding joint created by articulation of proximal & distal carpal rows ROM: Some extension, abduction, minimal rotation
Osseous structures - joints • Intercarpal: Gliding joints created by interface of individual carpal bones ROM: Complex • Carpometacarpal - First CMC (thumb base): Saddle joint, highly mobile; ROM: Flexion, extension, abduction, adduction, circumduction, rotation, opposition - Intermetacarpals 2nd-5th: Gliding joints; ROM: Limited mobility of 2nd & 3rd CMC, increasing mobility of 4th & 5th CMC
Good evaluation for integrity of scapho-lunate, lunotriquetral ligaments & TFC • Limited value for extrinsic ligaments • Injections spaced to allow contrast resorption • Radiocarpaljoint injected first (most likely to document with single injection); • If no tear, wait 30-60 minutes & proceed sequentially with distal radio-ulnar and midcarpalinjection • Digital subtraction allows dynamic evaluation of ligament status and sequential compartment injection without delay • Injectate: Iodinated contrast (180-300 mg I/ml); • Volumes: Midcarpal, 4-5 cc; radiocarpal, 2-3 cc; DRU, 1-2 cc; pisotriquetral, 1-2 cc Arthrography
Intact radiocarpal compartment - contrast filling pisotriquetral joint via prestyloid recess. Triangular fibrocartilage distal surface is outlined. Scapholunate& lunotriquetral ligaments are intact, with no evidence of spill into midcarpaljoint. Arthrograms
Radial tilt The normal distal radius angulation Normal = 16-28’ Abn = fracture likely Radiographic measurements
Lunate overhang: At least 50% of the lunate articular surface should articulate with the radial articular surface Radiographic measurements
Ulnar variance refers to length of distal ulna relative to distal radius • Ulnar minus: Ulna> 2 mm shorter than radius • Ulnar plus: ulna longer than radius Radiographic measurements
Volar bursae: Ulnar and radial sheaths Common flexor tendon sheath encases – index, middle, ring and little finger tendons Flexor pollics longs has a separate sheath Tendon sheaths - volar
Margins: • Dorsal margin = carpals • Volar margin = flexor retinaculum • Medial margin = pisiform & hook of the hamate • Lateral margin scaphoid & trapezium • Proximal margin = radiocarpaljoint • Distal margin = MC base Contents: • Flexor digitorumsuperficialis • Flexor digitorumprofundus • Median nerve Carpal tunnel - margins
Margins: Ventral margin = Superficial flexor retinaculum Median margin = Pisiform and Flexor carpi ulnaris Dorsolateral margin = Deep flexor retinaculum Contents: Ulnar artery & vein, Ulnar nerve Guyon canal
Margins: • Distal radius (proximal margin) • Extensor pollicuslongus(dorsal margin) • Adductor pollicuslongus& Extensor pollicusbrevis(volar margin) • APL & EPB converge just distal to 1st CMC (distal margin) • scaphoid, trapezium, 1st CMC & radial styloid (deep margin) Contents: • Cephalic vein • radial nerve • radial artery Tendons – anatomical snuff box
The term "triangular fibrocartilage complex of the wrist" was first coined by Palmer and Werner in 1981,1 Describes the cartilaginous and ligamentous structures that bridge the distal radius and ulna, Provides articulation with the adjacent lunate and triquetrum. Important stabilizer of the distal radioulnar joint Provides important shock absorption to the carpus. Triangular fibro-cartiliginous complex
The components of the TFCC include: The articular disc The dorsal and volar radioulnar ligaments The meniscus homologue The extensor carpi ulnaris tendon sheath The ulnocarpal ligaments TFCC
It is the articular disc and the radioulnar ligaments that are the most important to evaluate. Characteristic triangular shape The articular disc may be only 1-2 millimeters thick within its central portion, but the TFC thickens considerably at its dorsal and volar aspects, as well as at the ulnar attachments. The thickened dorsal and volar components are what comprise the dorsal and volar radioulnar ligaments. TFCC
A 3D depiction of the TFC (arrow) demonstrates its triangular shape and relatively thin central region. TFC Viewed from above, the thickened peripheral components that represent the dorsal and volar radioulnar ligaments (arrows) are readily apparent.
A T1-weighted coronal image demonstrates a normal TFC. Normal intermediate signal intensity is evident at the ulnar attachment (arrow). The normal interface with articular cartilage at the radial side is also apparent (arrowhead), and should not be mistaken for a vertical tear. Normal tfc
Injuries to the TFCC are a frequent cause of ulnar sided wrist pain. • MRI allows accurate pre-treatment evaluation of patients with suspected TFCC pathology • Provides excellent characterization of TFCC tears and their associated wrist pathology. • Such information is invaluable for the proper management of patients with TFCC tears. TFCC – mri
Neurovascular structures Dorsal
Radial artery Origin: • Terminal branch of brachial artery Course: • Superficial to pronator quadratus • Continues dorsally around radial styloidprocess • Passes deep to APL & EPB • Across anatomic snuffbox & deep to EPL Neurovascular structures