Download
1 / 7
70 likes | 71 Views
Hereditary angioedema (HAE) is the deficiency or dysfunction of C1 esterase inhibitor (C1-INH). However, it may also occur due to either<br>increased activity of factor XII / estrogen levels or through an unidentified cause. It manifests the attacks of swelling involving the skin and<br>/ or the mucosa / sub mucosa of different organs. The attacks may be the result of a specific trigger or occur spontaneously. The intestinal<br>angioedema is clinically presented with moderate or severe abdominal pain, associated with nausea, vomiting, diarrhea and / or ascites,<br>and interpreted as an u201cacute abdomenu201d. The treatment is into three distinct phases: treatment for acute attacks, short-term prevention, and<br>long-term prophylaxis. The 26-year-old woman with food and medication allergy presents with thirteen-year history of recurrent abdominal<br>pain diffuse and associated with diarrhea, nausea and hands, lips and eyelids swelling. During this period, she did several exams and six<br>laparoscopies that only revealed a small amount of free intraperitoneal fluid. Biochemical testing performed at that time revealed the C1<br>esterase inhibitor, decreased protein level, and C4 level, and she was, then, diagnosed in adults with intestinal involvement with HAE.<br>After the adequate treatment and prophylaxis, she evolved with reduction of the number of attacks. The late diagnosis is associated with<br>high morbidity. Therefore, it is extremely important the recognition and investigation of HAE with involvement in intestinal patients with<br>recurrent attacks of unexplained abdominal pain.

E N D
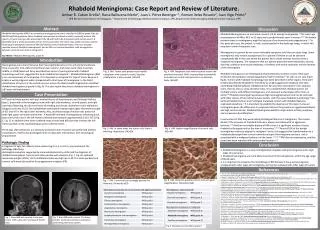
Journal of Gastroenterology & Digestive Systems Review Article Intestinal Angioedema: Case Report and Literature Review Zêmia Maria Câmara Costa Ferreira1, Anna Gabriela dos Santos Silva1, Fausto Daniel Mendes Morel1, Mayane Abrantes Veras de Freitas1, Irami Araújo-Neto1, Fabiana Lima Bezerra2, Silvio José de Lucena Dantas3, Amália Cinthia Meneses Rêgo4 and Irami Araújo-Filho5* 1Undergraduate student of the Medicine Course of the Potiguar University / UnP - Laureate International Universities; Student of Scientific Initiation; 2Ph.D in Biochemistry and Professor, Department of Microbiology and Parasitology, Federal University of Rio Grande do Norte / Brazil; *Corresponding author Dr. Irami Araújo-Filho, Department of Surgery, Federal University of Rio Grande do Norte. Full Professor, Department of Surgery, Potiguar University, PhD in Health Science. Natal - RN, 59020-650, Brazil, Ph No: +55 84 988760206; E-mail: irami.filho@uol.com.br 3Teacher of the Medicine Course of the Potiguar University / UnP- Laureate International Universities; 4Postgraduate Program in Biotechnology at Potiguar University/ UnP - Laureate International Universities; Pharmaceutical Biochemistry and Professor; Ph.D in Health Sciences; Submitted: 09 Aug 2018; Accepted: 15 Aug 2018; Published: 18 Aug 2018 5Postgraduate Program in Biotechnology at Potiguar University/ UnP - Laureate International Universities. Full Professor, Department of Surgery, Federal University of Rio Grande do Norte. Full Professor, Department of Surgery, Potiguar University. Ph.D in Health Science. Abstract Hereditary angioedema (HAE) is the deficiency or dysfunction of C1 esterase inhibitor (C1-INH). However, it may also occur due to either increased activity of factor XII / estrogen levels or through an unidentified cause. It manifests the attacks of swelling involving the skin and / or the mucosa / sub mucosa of different organs. The attacks may be the result of a specific trigger or occur spontaneously. The intestinal angioedema is clinically presented with moderate or severe abdominal pain, associated with nausea, vomiting, diarrhea and / or ascites, and interpreted as an “acute abdomen”. The treatment is into three distinct phases: treatment for acute attacks, short-term prevention, and long-term prophylaxis. The 26-year-old woman with food and medication allergy presents with thirteen-year history of recurrent abdominal pain diffuse and associated with diarrhea, nausea and hands, lips and eyelids swelling. During this period, she did several exams and six laparoscopies that only revealed a small amount of free intraperitoneal fluid. Biochemical testing performed at that time revealed the C1 esterase inhibitor, decreased protein level, and C4 level, and she was, then, diagnosed in adults with intestinal involvement with HAE. After the adequate treatment and prophylaxis, she evolved with reduction of the number of attacks. The late diagnosis is associated with high morbidity. Therefore, it is extremely important the recognition and investigation of HAE with involvement in intestinal patients with recurrent attacks of unexplained abdominal pain. Keywords: Angioedema, Hereditary Angioedema, C1 Esterase Inhibitor Deficiency, Complement C1 Inhibitor Protein, Gastrointestinal Diseases. Introduction Angioedema is characterized by edema, temporary location, and may reach the skin, Oropharynx, Airways, genital region and even the gastrointestinal tract. The intestinal angioedema is a less recognized and difficult to diagnose when compared to what affects the other parts of the body, due to your high rarity [1, 2]. surgical procedures and unnecessary treatments, thereby reducing the morbidity. In this sense, it is crucial to the knowledge that the episodes of angioedema may present with intestinal involvement and gastrointestinal clinical manifestations, whatever the triggering factor (inhibitors of angiotensin-converting enzyme, hereditary angioedema, among others) [3-5]. The Hereditary Angioedema (HAE) is a rare autosomal dominant disorder characterized by quantitative or functional deficiency of C1 Inhibitor (C1-INH) [6]. As a result, the individual presents episodes of edema in different organs. There are also reporting the association mutations in 20-25% of cases and the mutations of factor XII of the coagulation cascade. The detection and adequate treatment are fundamental for the good prognosis of the patient because it prevents this is subjected to J Gastro & Digestive Systems 2018 Volume 2| Issue 2 | 1 of 7
HAE presents itself into three distinct types. Most of the cases (80-85%) presents the HAE type I, characterized by low levels of C1-INH. Type II represents 15-20% of cases and is related to dysfunctional C1-INH, and at normal levels. Already the type III, with normal C1-INH is related to estrogen or factor XII mutation. There are also cases of idiopathic angioedema [4, 5-7]. of somatostatin, being all normal results. During most of the crises, the most relevant findings of laboratory tests were leukocytosis with neutrophilia and C-reactive protein (CRP) little high, which was not evidenced off the attacks of abdominal pain. In December 2017, intended to be hereditary angioedema diagnostic with intestinal involvement. CT scan with contrast was performed during the crisis that showed some slender handles hydroair distension. The dosage of C4 = 16 mg/dL (normal value: 19-52 mg/dL), C1 INH = quantitative 19mg/dL (normal value: 23-41 mg/dL) and C1q = 16.4 mg/dL (normal value: 10-25 mg/dL). The HAE is a misdiagnosed disease, due to your rarity and for not being known by many health professionals [3]. Its prevalence varies from 1:10,000 to 1:150,000. Patients present acute conditions for 20 to 100 days per year, representing between 15,000 and 30,000 emergency service visits annually [8-10]. The patient reported that she was promoted to a higher position in your job one year, which provided greater responsibility and stress. There was also started the practice of martial arts for one year (relationship with little trauma intensity). This period coincided with the increased incidence of crises. On the above, the present study consisted of a case report of angioedema hereditary, where they approached etiopathogenic characteristics, clinical presentation, diagnosis and treatment, in addition to a review of the literature on the topic [1]. During the follow-up, was a history of food allergies to seafood, pineapple and pepper, in addition to drug allergy to acetylsalicylic acid, dypirone, buscopan®, tramal®, dramine®, and no steroidal anti-inflammatory drugs (NSAIDS). The diet out of the crisis was restricted, out of food allergens. Was social and elitist denied smoking. Father is with a history of chronic diarrhea atopic. Maternal grandfather’s diagnosis of autoimmune pancreatitis. The patient made use of oral contraceptive Siblima® of 2008 the 2016 and Elane® of the 2016-2017. Methods The work presented here consisted of a literature review with the databases, PubMed/ Medline, Web of Science, Scielo, Lilacs and Scopus, using the following descriptors: hereditary angioedema, C1 esterase inhibitor deficiency, complement C1 inhibitor protein, digestive system, abdominal pain, edema, gastrointestinal diseases and laparoscopic surgeries. Ethics Committee The Research Ethics Committee of Pot Guar University – Natal/ Brazil, approved the research after signature by the patient informed consent, according to Resolution 466/2012, of the National Commission of Ethics and Research in Humans – CONEP – Ministry of Health/Brazil. Protocol number 547/2018. Currently, makes use of two capsules of Oxandrolone 25mg in the morning for treatment of the hereditary angioedema, with partial control of abdominal pain crises (decreased frequency). In December 2017, intended to be hereditary angioedema diagnostic with intestinal involvement. A new CT scan with contrast held during the crisis demonstrated hidroaérea distension a few slender handles. The determination of serum complement components showed reduced levels of C4=16 mg/dL (normal value: 19-52mg/ dL) and C1 INH=19mg/dL (normal value: 23-41 mg/dL), however the quantification of C1q=16.4 mg/dL (normal value: 10-25mg/dL) remained within the normality. Case Report Female, 26 years old, showed diffuse abdominal pain for 13 years, recurrent high intensity and sudden onset, colic, without precipitating factors aggravating or known. The pain was always associated with the diarrhea and, occasionally, nausea and vomiting. The bouts of pain lasted for about 3-5 days and to improve with the use of opioids, not having association with fever, chills, respiratory or urinary complaints. Associated with this syndromic status, the patient had swelling in hands, feet, lips and eyelids. Due to frequent evacuations during episodes of abdominal pain, was talking about weight loss. In the periods between crises, the abdominal pain was diffuse and of low intensity. Currently, makes use of two capsules of Oxandrolone, 25 mg in the morning for treatment of the hereditary angioedema, with partial control of abdominal pain crises (decreased frequency). Discussion Pathophysiology The hereditary angioedema (HAE) is a disease with heterogeneous characteristics and pathophysiology complex, which classifies into three distinct types: type I, II and III [11]. In order to standardize the nomenclature, it is possible to classify the HAE into three types: • Type I- HAE with quantitative C1-INH deficiency: there is a deficit greater than 50% in levels of C1-INH. Is the most prevalent phenotype (80-85% of cases) [9]; • Type II- HAE with C1-INH dysfunction: for normal levels of C1-INH, but committed functionality [10]; • Type III- HAE with C1-INH normal: this form predominates in female patients and is associated with serum levels of estrogen, such as pregnancy and exogenous administration, beyond the mutation in the gene encoding coagulation factor XII [8]. Until the definitive diagnosis of the disease, the patient underwent six laparoscopic procedures for diagnostic investigation of the clinical picture, due to the suspicion of acute abdomen. All surgeries have revealed the presence of free fluid in the peritoneal cavity and, in one of them, there was the presence of intestinal adhesion, which was removed. Performed laparoscopic appendectomy (2010) and cholecystectomy (2014) and, in both procedures, the samples were submitted to pathology, revealing, respectively, presence of edema without appendicitis and edema without cholecystitis or gallstones. In these periods, the findings of laboratory tests more relevant leukocytosis with neutrophilia and C-reactive protein (CRP) little high, which was not evidenced off the attacks of abdominal pain. In 2015, performed magnetic resonance imaging of the abdomen, colonoscopy, enteroscopy and whole body scintigraphy with analog J Gastro & Digestive Systems 2018 Volume 2| Issue 2 | 2 of 7
The HAE type I and II are termed hereditary angioedema associated with C1-Inhibitor (C1-INH-AHE), since they are caused by mutations in the SERPING 1 gene, which encodes the C1 esterase inhibitor (C1-INH). In type III or hereditary angioedema with C1 Inhibitor (AHE-C1n), 25% of cases are associated with mutations in the gene F12 coagulation factor XII encoder, in the other the pathogenesis remains unknown, although in some patients to be assigned to the exposure to estrogens (contraceptives or hormone replacement therapy) [11, 12]. There is no clinical improvement with the use of antihistamines, corticosteroids, or epinephrine, what differentiates the angioedemas mediated by histamine23. The duration of episodes of HAE in the patient ranged from 36 to 72 hours, not improving with the use of antihistamines [15]. About abdominal manifestations of the disease, they may come up to 93% of patients with HAE and involve edema in the intestinal handles. Characterized by severe abdominal pain, accompanied by nausea, vomiting, diarrhea, and ascites, mimicking acute abdomen [23-26]. Due to this similarity with acute abdomen, often leads to abdominal exploratory surgery. As a result, approximately one third of patients with undiagnosed HAE undergo unnecessary surgeries at the time of an abdominal attack [1]. Just as occurred in the case in question: patient submitted to six laparoscopic procedures, finding only free liquid in the cavity (ascites), occasions when it was submitted to appendectomy and cholecystectomy without diagnostic elucidation. So far, more than 200 mutations associated with HAE. In 75% of cases, mutations have an autosomal dominant pattern and in 25% the disease is the result of spontaneous mutations [13, 14]. In Hereditary Angioedema due to C1-Inhibitor, the SERPING 1 gene mutations may result in a quantitative reduction of the plasma levels of C1-INH, characterizing the type I of HAE, or cause a functional change of this inhibitor, sorting the HAE in Type II. The first is the most common phenotype, including 80-85% of cases. The HAE type II changes to the SERPING 1 gene results in the expression of normal levels of C1-INH, but generate a non-functional protein. Although, it is clinically similar to HAE type I, is less frequent (15- 20%) [11]. In both types of C4 serum levels are reduced and the C1q are normal, but what sets them apart is the amount of C1-INH [15]. When the HAE manifests with involvement of upper airway is more serious, because it can lead to suffocation and death if not treated in time [22, 27]. Crises can occur spontaneously or triggering factors: trauma (even that of small intensity), stress, infection, menstruation, pregnancy, alcohol consumption, invasive procedures (endoscopy, surgery, procedures dental procedures), extreme temperature changes, use of angiotensin-converting enzyme inhibitors and estrogen use [20, 23]. In this context, it is important to remember that the patient in question assumed a higher position in his job and started the practice of martial arts over the last year; was social and elitist by some years made use of oral estrogen-based birth control [28]. The C1-INH is a protein family of protease inhibitors, which act as inhibitor of serine proteases [16]. This protein binds irreversibly to C1r and C1s of the classical pathway of the complement system and MASP-1 and MASP-2 of the Mannose-binding lectin pathway. When interacting with these serine proteases, the C1-INH inhibits the early stages of both routes. Thus, in the absence of C1-INH, there is a greater consumption of C4, which justified a reduction in plasma levels of this protein in patients with HAE types I and II [17]. In addition to acting in the complement system, the C1-INH also promotes the inhibition of other proteases, such as plasma kallikrein and factor XII, which participate in the formation of bradykinin, final product via contact system activation [18]. The bradykinin is a peptide that stimulates the receptors vasoactive B2 of the endothelial cells, promoting the vasodilation and increased vascular permeability, which causes plasma extravasation to the interstitial and consequent angioedema [17]. In this context, the episodes of edema in HAE types I and II are caused by an overproduction of bradykinin, which is resulting from the quantitative or functional deficiency of C1-INH [9, 10]. Finally, some patients may show prodromal signs hours before the crisis, such as sensitive skin light changes (individual reports “strange feeling on the skin”), malaise, fatigue, mood changes and erythema marginatum [24-26]. Diagnosis When the episode of angioedema presents cutaneous manifestations or history of impairment of airway, which can occur in 50% of patients for at least one episode, it is more likely that this diagnosis is thought [27]. However, when the abdominal pain is the only clinical manifestation, it is common that the angioedema is not diagnosed or that this occurs only after multiple episodes of abdominal pain without obvious image examination findings [5]. It is important to note that more than one third of patients with intestinal angioedema are subjected to exploratory laparotomies or other unnecessary surgical procedures [6]. In these cases, rising morbidity and therefore the knowledge and early diagnosis of this disease is fundamental [1, 28]. In the clinical case presented, although the family history of the patient is not clear, the laboratory parameters (reduced levels of C1- INH and C4 and C1q normal amount) associated with your medical history, are compatible with a case of Angioedema Hereditary Type I. Clinical presentation Clinical history is of fundamental importance for the diagnosis of HAE. The symptoms have early onset, around 12 years of age, as occurred in the case reported in the table began to 13 years of age. Recurrent episodes of angioedema involving skin and asymmetrical sub mucosa of various organs. The regions most affected are: face, extremities, genitals, oropharynx, larynx and digestive system [19- 22]. The frequency and severity of crises are variables, where 5% of patients are asymptomatic and 25% present sporadic crises [20, 21]. It is essential that the clinician know that the episodes of HAE last around 48 to 72 hours, when they do not receive proper treatment. One of the symptoms that can raise the suspicion of HAE, include edema of larynx, subcutaneous edema and/or sub mucosa without associated rash that can occur anywhere in the body; abdominal pain; nausea; vomiting and diarrhea [29, 30]. The history and physical examination are essential for the diagnosis, in addition to exclude other causes of acute abdomen [10]. On clinical history should try to identify triggers and describe as crises occur, how long they last, if there are and what are the factors of J Gastro & Digestive Systems 2018 Volume 2| Issue 2 | 3 of 7
improvement and worsening of syndromic framework, age of the first episode and duration of the interval between crises, in addition to the signs and symptoms present in those time slots [5, 23-26]. Individuals with values of C1-INH within the range of normal (normal = 25-41mg/dL) and positive family history to HAE, besides positive medical history, are classified with HAE with normal C1- INH. For those who exhibit C4 value normal, due to quantitate the amount of C1-INH, and below the normal range, HAE is defined as quantitative C1-INH deficiency [34]. If the number of C1-INH test is normal, the qualitative test should be performed (normal activity is 70-130%, being the value less than 50% accepted for diagnosis) and, if reduced, the individual is framed in HAE with C1-INH [1-3]. In addition to the characterization of the episode algic, it is necessary to investigate the use of medications that raise levels of bradykinin (angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, gliptins), as well as use of medicines involved with the biggest factor XII gene and expression of B2 receptors such as estrogen (estrogen contraceptives and hormone replacement therapy), and medications that may be involved in differential diagnosis of abdominal pain, as the NSAIDS [5, 6]. It is essential to investigate the possible triggering factors and family history that can be positive in up to 75% of cases [31]. With the C4 and C1-INH dosing also changed, you need to evaluate the value of C1q, metabolic product related to angioedema associated with lymph proliferative or autoimmune processes (acquired angioedema with C1-INH deficiency). In this type of angioedema, C1q value is low, different from what occurs in the case of HAE, where there is no change to the C1q [1, 17]. The patient featured C4 and C1-INH reduced with C1q within the range of normality away from the possibility of angioedema associated with lymph proliferative or autoimmune processes. In relation to the physical exam, this can be changed only during the acute crisis and especially to the skin changes, with no prickly edema or hives showing up as typical manifestations [8, 27]. The examinations of the tongue, lips and oral cavity are critical. There needs to be a special attention to the signs and symptoms of respiratory distress, such as stridor. Abdominal involvement is nonspecific, expressing themselves with diffuse pain, peritoneal irritation and the presence or not of the sign of rebound [5, 32]. In acquired angioedema with C1-INH deficiency associated with the autoimmune disease, the reduction in levels of C1-INH is explained mainly by the presence of antibodies against this inhibitor [1, 30-32]. In relation to specific laboratory changes, episodes of abdominal crisis can attend with leukocytosis with neutrophilia associated with increasing the level of hematocrit, once these levels greater than outside the abdominal pain or angioedema without abdominal involvement. However, the C-reactive protein (CRP) generally remains low even during the bouts of intestinal angioedema [33]. As for the differential diagnosis, it is important to make the distinction between HAE and angioedemas chronic histaminergic. For that, it can be a therapeutic test with antihistamines, using up to four times the usual dose for six weeks and then the response of the individual to the test [35]. Antihistamines are safer to carry out are cetirizine, desloratadine, fexofenadine, levocetirizine and rupatadine. If the person does not submit response to therapeutic testing and other causes of angioedema have been excluded, the diagnosis of angioedema not-idiopathic histaminérgico [5, 36]. With regard to imaging scans, computed tomography (CT), ultrasound (USG), nuclear magnetic resonance (NMR) and the x-ray show nonspecific signs. Ascites, bowel edema with dilatation of handles and invaginations in “finger gloves” are suggestive and displayed during the crisis [22-24]. Upper gastrointestinal endoscopy is not recommended because of the risk of inducing laryngeal edema by local trauma and cause respiratory distress. However, if held, could demonstrate mucous edema, erythema and cambers gastric mucosal site [7-9]. Treatment The management of the HAE is in control of the symptomatology in three great moments: crisis, prophylaxis of short term and long- term prophylaxis. Among the general guidelines, education and guidance have highlighted. The patient must receive relevant information about your disease, preventive measures and action plans for crises. Are necessary for the identification and elimination of triggers, such as stress, trauma and the use of some medications or inductors which prolong the crisis. Is recommended the maintenance of up-to-date vaccination, particularly against hepatitis A and B [31-34]. As for the diagnostic criteria, they are divided into major, secondary and biochemical [2-4]. The greater presence of angioedema not subcutaneous inflammatory lasting 12:00, abdominal pain of indefinite etiology lasting six hours and laryngeal edema; the secondary criteria are a family history of angioedema visceral; and biochemical criteria are quantitative deficiency of C1-INH < 50% in two separate samples of functional C1-INH deficiency < 50% in two separate samples. The diagnosis is confirmed in the presence of a larger criterion and a biochemist. However, when there is high suspicion of HAE and complement dosages are inconclusive, you can perform genetic testing to evaluate the presence of mutation in the gene SERPING1, C1-INH encoder [21, 33]. During the crisis, the treatment depends on the severity. The classification as regards the gravity is defined as follows: mild, if there is no limitation in the implementation of daily activities; moderate, when does not prevent to do them, but the performance is impaired; and serious, when performing impossible [30, 37]. Serious crises and/or with involvement of airways need urgent approach. The priority, in this case, is the maintenance of the airways pervious and crisis therapy is to inhibit the synthesis of bradykinin and your action in the endothelium. We recommend an early venous access for IV rehydration and medication administration [23, 30]. Individuals with clinical suspicion or family history positive for HAE should be investigated. The determination of serum C4 can serve as screening: If the dosage is normal (between 17-45 mg/dL) and low clinical suspicion, HAE is discarded; If the dosage is normal associated with high clinical suspicion, should reap examinations in time of crisis, along with the dosage of C1-INH [8-11]. The drug treatment consists of three pharmacological therapies considered first line: pdC1-INH concentrate, Icatibant and J Gastro & Digestive Systems 2018 Volume 2| Issue 2 | 4 of 7
Ecallantide. The FFP comes in as second-line approach because, despite controlling most of the crises, has kininogen and kallikrein that can generate a paradoxical worsening the possibility of producing more bradykinin, in addition to the intrinsic risks to your use, such as the transfusion reactions [36-38]. Other ducts as volume replacement, analgesia and control of nausea are necessary for patient comfort and improved morbidity associated with [5]. day), divided into 2 to 3 taken, 5 days before and 2-5 days after the procedure [5]. Long-term prophylaxis already aims to reduce the frequency and severity of crises. She is reserved for individuals with frequent symptoms that affect upper airways or to cause substantial emotional or physical incapacitation [23]. However, there is still no well- established consensus about the number of crises or the severity of episodes that define the indication of this type of prophylaxis. However, individuals who exhibit more of a serious crisis by month are strong candidates to be benefited with this therapeutic approach [5, 39]. Antifibrinolytics androgens and are not recommended for the control of the crisis due to the delay in your early action [3]. Within the Group of C1-INH concentrates, the options are Berinet®, pasteurized concentrate nanoformulated, administered at a dose of 20U/Kg, intravenously and that can be administered the household level; Cinryze®, pdC1-INH concentrate nanoformulated, used at a dose of 1000U, IV, repeated after 1 hour the first administration; Ruconest®, recombinant C1-INH obtained from the milk of transgenic rabbits, which recommended dose 50U/Kg, if the individual has less than 185 pounds, or 4200U for adults weighing more than 185 pounds [5, 36]. Attenuated androgens (Danazol, Estanazolol and Oxandrolone) are the medication of choice for long-term prophylaxis. They act in two ways: increase the synthesis of C4, which regulates the complement system, reducing consumption of C1-INH and the synthesis of C1- INH due to anabolic effect [30]. For your use, it is important to the accompaniment of the lipid profile, blood count, liver enzymes, alpha-fetoprotein and contents of urine, in addition to abdominal ultrasound for evaluation of liver echography annually [27]. If the individual evolves with dyslipidemia or liver damage, the dose should be reduced or your use should be discontinued until clinical improvement. Attenuated androgen therapy is contraindicated in pregnant women, children and in cases of adverse reactions: weight gain, virilization, irregular menstrual cycle, headache, depression and hepatic adenoma [29-31]. The Icatibant (Firazyr®) is a competitive antagonist of bradykinin B2 receptor, recommended in the first 6h at a dose of 30mg subcutaneous tissue. The dose can be repeated up to three times in 24h (10% of crises require a second dose). Its use is only recommended for patients older than 18 years [4-6, 35]. The Ecallantide (Kalbitor®) is an inhibitor of cralicrein the genesis of bradykinin. Used at a dose of 30mg, subcutaneously. Is not approved for home use because of the risk of anaphylaxis, observed in up to 3% of cases [2]. Among the attenuated androgens, Danazol is the most widely used. Your maximum dose is 200mg/day and, if we do not reach the desired effect even with the recommended maximum, you can associate the use of antifibrinolytics agents. Oxandrolone may be used in adults, at a dose of up to 2, 5 mg every 8-12h (maximum 20 mg) and, in children, 0,25mg/Kg/day, the Estanazolol can be used up to 2mg/ day [29, 30]. Short-term prophylaxis should be made when it is necessary to submit the patient to any condition that may lead to crisis, as surgery (especially in cervicofacial region or who require tracheal intubation) and dental procedures [8-10]. In relation to agents antifibrinolytics (Epsilon-Aminocaproic acid and tranexamic acid), they are the second class of medications of the long-term prophylaxis, being effective in crisis prevention by up to a third of patients. Act antagonizing the fibrinolytic system, block the formation of plasmin and inhibit proteolytic activity of plasminogen activators1-3. How do not alter serum levels of C1- INH, are good choice for patients with HAE and normal C1-INH. Before recommending your use, it is necessary to perform liver function tests and research of history of thromboembolic disease personal and family [4]. If the individual is subjected to a low-risk procedure, must, first of all, evaluate whether there is treatment for a crisis available [11]. If so, it will be submitted to the procedure under strict observation and, in the event of a crisis, the approach must be made immediately as already mentioned [24]. If there is availability for the treatment of the crisis, should be administered prophylactically attenuated androgen [3]. When it comes to a high-risk procedure or that is necessary to tracheal intubation, should administer C1-INH concentrate. If he is not available, alternatively attenuated androgens and/or fresh plasma [1, 2]. The therapeutic agent of choice in this class, due to the higher power and lower side effects, is tranexamic acid made at a dose of 20-50mg/Kg/day (maximum of 4-6 g/day), orally, in 2-3times/day. The second option is the Epsilon-Aminocaproic acid, until 6-8 g/ day orally divided into 2-4 times/day in adults and 100-200mg/Kg, orally, in 3-4 times/day in children [5, 31, 36]. For short-term prophylaxis, doses of packed pdC1-INH are the same as for acute situations. Fresh-frozen plasma should be administered at a dose of 10 ml/Kg and the attenuated androgen Danazol is suggested, at a dose of 10mg/Kg/day (maximum 600mg), divided into 3 taken daily during 5-7 days before and 2 days after the procedure [37, 38]. The third classes of long-term prophylaxis are the pdC1-INH concentrates. Are safe and effective options. Used every 3-4 days. However, due to the need for venous access and your high cost, are indicated when the individual has reduced the quality of life, severe acute episodes and frequent, therapeutic failures or intolerance to androgens [5, 37-39]. In respect of antifibrinolytics agents, as there is no proven effectiveness, your use should be reserved for situations in which none of the previous options are available. Tranexamic acid is the most widely used, at a dose of 25mg/Kg/day (maximum 3-6 g/ J Gastro & Digestive Systems 2018 Volume 2| Issue 2 | 5 of 7
It is important to note that, in cases of HAE in childhood, antifibrinolytics agents present themselves as first choice in long-term prophylaxis, since the use of attenuated androgens are contraindicated because they induce the early closure of the plates Introduction epiphyseal [21, 22]. The FFP is an option in prophylaxis of short duration, if there is no availability of packed pdC1-INH or the patient is less than 12 years [8-10, 30]. Angioedema Revisited. Clin Rev Allergy Immunol 51: 170-182. 12. Grigoriadou S, Longhurst HJ (2009) Clinical Immunology Review Series: An approach to patient with angio-oedema. Clin Exp Immunol 155: 367-377. 13. Cugno M, Zanichelli A, Foieni F, Caccia S, Cicardi M (2009) C1-inhibitor deficiency and angioedema: molecular mechanisms and clinical progress. Trends Mol Med 15: 69-78. 14. Ali MA, Borum ML (2014) hereditary angioedema: what the gastroenterologist needs to know. Clin Exp Gastroenterol 7: 435-445. 15. Bowen T, Cicardi M, Farkas H, Bork K, Longhurst HJ, et al. (2010) 2010 International consensus algorithm for the diagnosis, therapy and management of hereditary angioedema. Allergy Asthma Clin Immunol 6: 24. 16. Bos IG, Hack CE, Abrahams JP (2002) Structural and functional aspects of C1-inhibitor. Immunobiology 205: 518-33. 17. Kaplan AP, Joseph K (2017) Pathogenesis of Hereditary Angioedema: The Role of the Bradykinin-Forming Cascade. Immunol Allergy Clin North Am 37: 513-525. 18. Hofman Z, de Maat S, Hack CE, Maas C (2016) Bradykinin: Inflammatory Product of the Coagulation System. Clin Rev Allergy Immunol 51:152-161. 19. Bygum A, Andersen KE, Mikkelsen CS (2009) Self- administration of intravenous C1-inhibitor therapy for hereditary angioedema and associated quality of life benefits. Eur J Dermatol 19: 147-151. 20. Kaplan AP, Joseph K (2014) Pathogenic mechanisms of bradykinin mediated diseases: dysregulation of an innate inflammatory pathway. Adv Immunol 121: 41-89. 21. Silva MR, Beraldo WT, Rosenfeld G (1949) Bradykinin, a hypotensive and smooth muscle stimulating factor released from plasma globulin by snake venoms and by trypsin. Am J Physiol 156: 261-273. 22. Elliott DF, Horton EW, Lewis GP (1960) Actions of pure bradykinin. J Physiol 153: 473-480. 23. Zuraw BL, Herschbach J (2000) Detection of C1 inhibitor mutations in patients with hereditary angioedema. J AllergyClinImmunol 105: 541-546. 24. Ohsawa I, Honda D, Nagamachi S, Hisada A, Shimamoto M, et al. (2014) Clinical and laboratory characteristics that differentiate hereditary angioedema in 72 patients with angioedema. Allergol Int 63: 595-602. 25. Zuraw BL, Banerji A, Bernstein JA, Busse PJ, Christiansen SC, et al. (2013) US Hereditary Angioedema Association Medical Advisory Board. US Hereditary Angioedema Association Medical Advisory Board 2013 recommendations for the management of hereditary angioedema due to C1 inhibitor deficiency. J Allergy Clin Immunol Pract 1: 458-467. 26. Bowen B, Hawk JJ, Sibunka S, Hovick S, Weiler JM (2001) A review of the reported defects in the human C1 esterase inhibitor gene producing hereditary angioedema including four new mutations. ClinImmunol 98: 157-163. 27. Lunn ML, Santos CB, Craig TJ (2010) is there a need for clinical guidelines in the United States for the diagnosis of hereditary angioedema and the screening of family members of affected patients? Ann Allergy Asthma Immunol 104: 211-214. 28. Bork K, Meng G, Staubach P, Hardt J (2006) Hereditary Angioedema: New Findings Concerning Symptoms, Affected Organs, and Course. Am J Med 119: 267-274. 29. Craig T (2012) WAO Guideline for the Management of Hereditary Angioedema. WAO Journal 5: 182-199. In the cases of pregnant women with HAE, the long-term prophylaxis with attenuated androgens is not recommended, because they cross the placental barrier and can cause virilization of fetus [18-20]. The use of tranexamic acid should also be avoided as it also crosses the placental barrier, although cause fewer side effects [36-39]. The pdC1-INH concentrate, in these cases, is the first choice, administered at a dose of 500/2000U-week [5-7, 22]. Conclusion In conclusion, it is essential to know the clinical picture and the complementary tests that aid in the diagnosis and treatment of Hereditary Angioedema, since the morbimortality of the patients increases with the time of disease, altering the quality of life of patients and their families. Such conduct avoids numerous visits to emergency services and submission to unnecessary diagnostic and therapeutic procedures, as about one-third of patients with HAE may undergo unnecessary abdominal surgeries. Conflict of interest statement The authors have no conflicts of interest to declare. References 1. Nzeako UC (2010) Diagnosis and management of angioedema with abdominal involvement: A gastroenterology perspective. World J Gastroenterol 16: 4913-4921. 2. Giavina-Bianchi P, Kalil J (2018) Improving the Management of Hereditary Angioedema. Clinics (Sao Paulo) 73: e354. 3. Locascio EJ, Mahler S, Arnold TC (2010) Intestinal Angioedema Misdiagnosed as Recurrent Episodes of Gastroenteritis. West J Emerg Med 4: 391-394. 4. Banerji A (2011) hereditary angioedema: Classification, pathogenesis, and diagnosis. Allergy Asthma Proc 32: 403-407. 5. Sochal M, Gabryelska A, Kowalski MK, Biernacka K, Lewandowska-Polak A, et al. (2018) Hereditary angioedema restricted to the digestive tract. Prz Gastroenterol 13: 80-81. 6. Reshef A, Leibovich I, Goren A (2008) Hereditary angioedema: New hopes for an orphan disease. Isr Med Assoc J 10:850-855. 7. Loules G, Zamanakou M, Parsopoulou F, Vatsiou S, Psarros F, et al. (2018) Targeted next-generation sequencing for the molecular diagnosis of hereditary angioedema due to C1- inhibitor deficiency. Gene 1119: 30512-30522. 8. Zuraw BL, Christiansen SC (2016) HAE Pathophysiology and Underlying Mechanisms. ClinRev Allergy Immunol 51: 216-229. 9. Giavina-bianchi P, L Karla Arruda, Marcelo V Aun, Regis A Campos, Herberto J Chong-Neto, et al. (2010) Diretrizes do diagnóstico e tratamento do angioedema hereditário. Revista Brasileira de Alergia e Imunopatologia 33: 241-251. 10. Lumry WR, Castaldo AJ, Vernon MK, Blaustein MB, Wilson DA, et al. (2010) the humanistic burden of hereditary angioedema: Impact on health-related quality of life, productivity, and depression. Allergy AsthmaProc 31: 407-414. 11. Germenis AE, Speletas M (2016) Genetics of Hereditary J Gastro & Digestive Systems 2018 Volume 2| Issue 2 | 6 of 7
30. Bork K, Hardt J, Witzke G (2012) fatal laryngeal attacks and mortality in hereditary angioedema due to C1-INH deficiency. J Allergy Clin Immunol 130: 692-697. 31. Agostoni A, Cicardi M (1992) Hereditary and acquired C1- inhibitordeficiency: biological and clinical characteristics in 235 patients. Medicine (Baltimore) 71: 206-215. 32. Longhurst H, Cicardi M (2012) Hereditary angio-oedema. Lancet 379: 474-481. 33. Ferraro M, Moreno A, Castelli E, Donadi E, Palma MS, et al. (2011) A single nucleotide deletion at the C1 inhibitor gene as the cause of hereditary angioedema: insights from a Brazilian family. Allergy 66: 1384-1390. 34. Jalaj S, Scolapio JS (2013) Gastrointestinal Manifestations, Diagnosis, and Management of Hereditary Angioedema. J ClinGastroenterol 47. 35. Zeerleder S, Levi M (2016) Hereditary and acquired C1- inhibitor-dependent angioedema: from pathophysiology to treatment. Ann Med 48: 256-267. 36. Fabiani JE (1990) Angioedema hereditário (AEH) acción del danazol sobre el C4 y C1-INH funcional. 37. Cicardi M, Bork K, Caballero T, Craig T, Li HH, et al. (2012) Evidence-based recommendations for the therapeutic management of angioedema owing to hereditary C1 inhibitor deficiency: consensus report of an International Working Group. Allergy 67: 147-157. 38. Horiuchi T, Hiroyuki Ohi, Isao Ohsawa, Teizo Fujita, Misao Matsushita, et al. (2012) Guideline for Hereditary Angioedema (HAE). Allergology International 61: 556-559. 39. Ohsawa I, Nagamachi S, Suzuki H, Honda D, Sato N, et al. (2013) Leukocytosis and high hematocrit levels during abdominal attacks of hereditary angioedema. BMC Gastroenterology 13: 123. Copyright: ©2018 Irami Araújo-Filho, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. J Gastro & Digestive Systems 2018 Volume 2| Issue 2 | 7 of 7