Download
1 / 45
450 likes | 763 Views
Urological Cancer. Kieran Jefferson Consultant Urological Surgeon University Hospital, Coventry. Recommended Texts. Urology – a handbook for medical students Brewster, Cranston et al Oxford Handbook of Urology Similar authors, more postgraduate. Two-week wait urology. Haematuria –

E N D
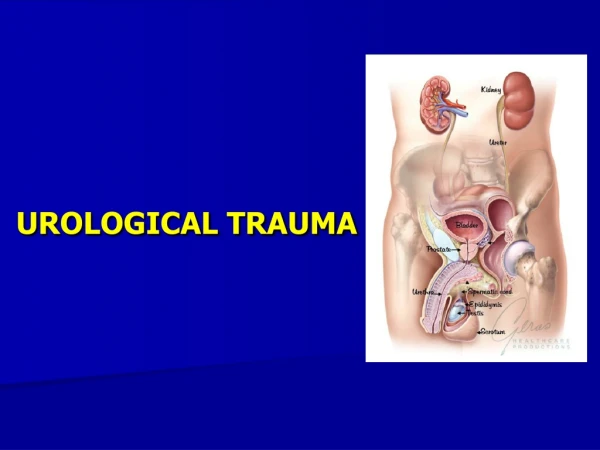
Urological Cancer Kieran Jefferson Consultant Urological Surgeon University Hospital, Coventry
Recommended Texts • Urology – a handbook for medical students • Brewster, Cranston et al • Oxford Handbook of Urology • Similar authors, more postgraduate
Two-week wait urology • Haematuria – • frank/microscopic over 50 years old • Raised PSA/abnormal DRE • Mass in body of testis • Renal mass on imaging/palpation • Any suspicious penile lesion
Haematuria • Common, major challenge for urologists • Visible haematuria 20% chance cancer • Microscopic haematuria 5-10% chance
Causes of haematuria • Infection • Benign prostatic hypertrophy • Malignancy • bladder, kidney, ureter, prostate • Stone • bladder, ureter, kidney • Glomerulonephritis • IgA nephropathy • Trauma
Management • History and examination • Investigations • Treatment
History • Type, duration, associated LUTS or pain • Medication • Anticoagulants • nephrotoxins • Medical/surgical history • stone or previous surgery • SHx • Smoking, chemical exposure, employment
Examination • Stigmata of renal disease • Hypertension • Oedema • Abdomino-pelvic masses/scars
Investigations • Ideally as part of ‘one-stop’ haematuria clinic • MSU dipstix, M,C&S, cytology • FBC, U&Es • Flexible cystoscopy • USS renal tract +/- or contrast CT
Treatment • As per aetiology
Bladder cancer • 4th commonest male/10th commonest female cancer • Risk Factors • Age, sex • Smoking, exposure to benzene compounds • Drugs – phenacetin, cyclophosphamide
Bladder cancer subtypes • Primary • Transitional cell carcinoma • Squamous cell carcinoma • Adenocarcinoma • Sarcoma • Secondary
Presentation • Symptoms/signs from primary or secondary tumours +/- paraneoplastic phenomena • Haematuria, dysuria, frequency/urgency • Ureteric obstruction
Management • As for all cancers, dependent on stage and grade of tumour and co-morbidities • TCCs described as GxTy (grade/TNM stage) • Can be either curative or palliative
Diagnosis/staging • Clinical diagnosis usually made at flexi cysto • TURBT (including VE or DRE) to establish tissue diagnosis, then Mitomycin • If tissue stage pT2 or greater, staging CT chest/abdo/pelvis
Treatment • Superficial TCC (pT<2) • TURBT followed by regular review flexi cystoscopy • Intravesical treatment with mitomycin or bCG if high grade or multiply recurrent • Recurrent high grade disease merits consideration of cystectomy • Invasive TCC or other subtypes • Radical surgery or radiotherapy after neoadjuvant chemotherapy if cure possible • Palliative surgery/radiotherapy/medical symptom control
Prognosis • Superficial TCC – excellent unless high-grade • Invasive TCC – approx 50% overall 5y/s • Metastatic – extremely poor
Renal cell cancer • UK 7000 cases; 3600 deaths/year • 3% all cancer • Mortality is NOT declining • >50% incidental findings on imaging • 30% present with metastases
Clinical Features • Asymptomatic (>50%) • Haematuria • Flank Pain • Mass • Metastatic/paraneoplastic
Paraneoplastic Syndromes • Anaemia (>30%) • Erythrocytosis (3%) • Cachexia • Hepatic dysfunction • Hormonal abnormalities • Hypercalcaemia
Metastases • Lung • Bone • Liver • Brain
Management • Dependent on stage, grade & co-morbidity! • Curative vs palliative • Only curative option is surgery • Laparoscopic radical nephrectomy • Lap/open partial nephrectomy • Palliation with TKIs and mTOR antagonists
Prognosis • Good if resectable primary tumour • Very poor for metastatic disease
Prostate cancer • Commonest solid tumour in UK males • 35000 cases & 10000 deaths per year • Risk factors • Age, male sex • Significantly less common in oriental races
Pathology • Adenocarcinoma is commonest form (95%+) • Gleason Grading system • Sum of two commonest morphologies
Presentation • Asymptomatic • raised PSA/opportunistic DRE • LUTS, lymphoedema, PE/DVT, ureteric obstruction/ARF, haematuria, impotence • Bone pain, anaemia, sclerotic bone on XR
Management • Dependent on stage, grade & co-morbidity! • History & Examination • PSA, U/Es, FBC • Truss-guided prostate biopsy • Isotope bone scan/MRI prostate
Selecting treatment • Not all tumours warrant treatment (morbidity of treatment outweighs potential benefit to patient) • Whitmore’s conundrum • ‘Is it possible that no treatable prostate cancer requires treatment, but that all those requiring treatment are untreatable?’
Treatment options • Curative (radical) • Radical prostatectomy (open, laparoscopic, robotic) • Radical external beam radiotherapy • Brachytherapy • Palliative • Watchful waiting • Hormone ablation • Chemotherapy • Radiotherapy
‘The Third Way’ • Active surveillance • Aims to select out patients who will do badly and defer radical treatment until progression is imminent • Good evidence that rate of change of PSA correlates well with aggressiveness of tumour • Only immediate side-effect is psychological
Testicular cancer • Commonest solid tumour of young men • Commoner in European populations • Exceptionally good prognosis due to effective platinum-based chemotherapy
Pathology • Germ cell tumours (95%) • Seminoma, teratoma • Sertoli cell tumours • Leydig cell tumours • Lymphomas (older men)
Presentation • Painless testicular lump • Pain from infarction/infection/trauma • Symptomatic metastases • Retroperitoneal lymph nodes (varicocoele) • Lungs, bones
Management • Dependent on stage, grade & co-morbidity! • But • Almost all are potentially curable • Co-morbidity is uncommon in these men
Assessment • History & Examination • Serum Tumour Markers • Αlpha-foetoprotein (AFP) • ß-human chorionic gonadotrophin (hCG) • Lactate dehydrogenase (LDH) • Radical orchidectomy for histology followed by CT chest/abdo/pelvis
Oncological management • Most now get chemotherapy • Platinum-based • Some also radiotherapy and retroperitoneal lymph node dissection • Vast majority are cured but need regular imaging and risk second Ca
Penile cancer • Rare (in UK) • Association with HPV subtypes (cf cervical cancer) • Any suspicious lesion on glans or prepuce warrants early referral if fails to respond to steroids • Squamous tumours usually treated surgically, some role for radiotherapy/chemo