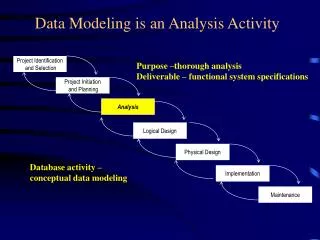
Download
1 / 30
390 likes | 820 Views
Ibrutinib: Analysis of Pivotal Data. Richard R. Furman, MD CLL Research Center. BCR-associated Kinases: Proven Effective Therapeutic Targets. Syk (spleen tyrosine kinase ): fostamatinib PRT062070 GS-9973. Btk (Bruton’s tyrosine kinase): ibrutinib CC-292 ACP-196 ONO-4059.

E N D
Ibrutinib: Analysis of Pivotal Data Richard R. Furman, MD CLL Research Center
BCR-associated Kinases:Proven Effective Therapeutic Targets • Syk (spleen tyrosine kinase): • fostamatinib • PRT062070 • GS-9973 • Btk (Bruton’s tyrosine kinase): • ibrutinib • CC-292 • ACP-196 • ONO-4059 • PI3K (phosphatidyl 3-kinase): • Idelalisib (GS-1101) • Duvelisib (IPI-145) • AMG319 Nat Rev Immunol 2:945
Issues with Novel Agents Response Criteria • Redefine clinical endpoints • Evolution of response over time Dosing: • No more MTD dosing • Threshold dosing • Fixed dosing / wide therapeutic window Re-evaluation of Prognostic Markers Re-evaluation of MRD
Redefining Clinical End Points“Cheson 2012” Standard response criteria: measure of treatment efficacy Need to provide means for determining need for treatment discontinuation For novel agents, response criteria don’t measure effect: • Thalidomide / lenalidomide: tumor flare • BCR Antagonists: lymphocytosis (Not tumor flare) Cheson BD. JCO 2012;30:2820.
Cheson 2012: Recommendations For IMIDs: Assessment of PD should use repeat observations and incorporate indicators of PD not associated with tumor flares. For BCR-targeted agents: lymphocytosis alone should not be considered an indicator of PD. Need to demonstrate other CLL-related signs or symptoms of PD. Lymphocytosis is distinct from tumor flare
Evolution of Responses Over Time:Kinase Inhibitors • Achievement of best response was time dependent • Proportion with CR/PR increased during follow-up • Proportion with PR+L diminished as the lymphocyte count declined over time
Issues with Novel Agents Response Criteria • Redefine clinical endpoints • Evolution of response over time Dosing: • No more MTD dosing • Threshold dosing • Fixed dosing / wide therapeutic window Re-evaluation of Prognostic Markers Re-evaluation of MRD
Ibrutinib: Discovery Person Disease Enzyme Drug ibrutinib O NH2 N N N N N O Bruton’s Agammaglobulinemia, 1952 Bruton Tyrosine Kinase, 1993 Synthesized 2005 First in human 2009 1st approval 2013 Ogden Bruton (1908-2003)
Ibrutinib: Inhibitor of Bruton’s Tyrosine Kinase • Forms an irreversible bond with cysteine-481 in Btk • Potent Btk inhibition • IC50=0.5 nM • Orally bioavailable • Daily dosing resulting in 24-hr target inhibition • Possible impact on T-cells • Possible impact upon Tec, Bmx, Blk, Itk, and platelets O NH 2 N N N N N O
Phase I Study of Ibrutinib inB-Cell Malignancies Advani RH. JCO 2013;31(1):88.
IC50 Values of Ibrutinib and Related Kinases Honigberg LA. PNAS 2010; 107:13075.
BTK Inhibition and Plasma Levels Occupancy indicates irreversible inhibition of BTK Plasma concentration profile reflects inhibition profile of reversibly inhibited off targets
Ibrutinib Pivotal Study: RESONATE Oral ibrutinib 420 mg once daily until PD or unacceptable toxicity n=195 1:1 R ANDOM I Z E Crossover to ibrutinib420 mg once daily after IRC-confirmed PD (n=57) IV ofatumumab initial dose of 300 mg followed by 2000 mg × 11 doses over 24 weeks n=196 Eligibility: Relapsed and not appropriate for purine analog therapy: Disease progression < 3 years from prior purine analog Age >70 or age>65 with comorbidities Relapsed and deletion 17p purine analog associated AIHA / ITP Byrd JC. NEJM 2014; 371:213
RESONATE: Study Objectives Primary Objective • PFS as assessed by the IRC per 2008 IWCLL criteria with the 2012 clarification for treatment-related lymphocytosis • Secondary Objectives • Overall survival • IRC-assessed overall response rate • Safety and tolerability • Exploratory Objective • Investigator assessed progression free survival and overall response rate
RESONATE: Baseline Characteristics Byrd JC. NEJM 2014; 371:213
Patient Disposition Byrd JC. NEJM 2014; 371:213
RESONATE: Progression Free Survival 100 90 80 70 60 Progression-Free Survival (%) 50 40 30 20 10 0 0 3 6 9 12 15 Months No. at risk • Ibrutinib significantly prolonged PFS • 78% reduction in the risk of progression or death • Investigator assessed PFS hazard ratio 0.133 (95% CI: 0.085-0.209) p value < 0.0001 • Richter’s transformation was confirmed in 2 patients on each arm. An additional patient on the ibrutinib arm experienced disease transformation to prolymphocytic leukemia Ibrutinib: 195 183 116 38 7 Ofatumumab: 196 161 83 15 1 0
RESONATE: Overall Survival | | | | | | 100 | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | Ibrutinib (n=195, 16 events) | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | 90 | | | | | | Ofatumumab (n=196, 33 events) | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | 80 70 60 50 Overall Survival (%) 40 30 20 10 0 18 0 3 6 9 12 15 Month • Ibrutinib significantly prolonged OS compared with ofatumumab • This represents a 57% reduction in the risk of death for the ibrutinib arm • At the time of this analysis, 57 patients initially randomized to ofatumumab were crossed over to receive ibrutinib following IRC-confirmed PD
AE: Bleeding Resonate: all grades: 44% vs 12% grade 3-4: 1% vs 2% BTK and TEK modulate glycoprotein VI signaling following binding of collagen Three Studies: • Farooqui: PFA-100: epinephrine / ADP normal • Rushworth: aggregometry: collagen and ADP abnormal • no explanation for ADP findings • Kamel: aggregometry: collagen abnormal
AE: Diarrhea Possibily mediated by EGFR inhibition Reversible Only symptomatic with food in GI tract Take medication prior to bedtime
Conclusion Ibrutinib initially approved based upon phase II data for relapsed CLL patients who have received at least one prior therapy Based upon the RESONATE data, ibrutinib’s approval updated to include deletion 17p at any line of therapy Phase III data provided new insights into adverse events: atrial fibrillation Responses will evolve over time: STAY TUNED!