Download
1 / 27
530 likes | 2.39k Views
Bronchopulmonary Dysplasia. NICU Night Curriculum. Learning Objectives. To understand the clinical course and presentation of bronchopulmonary dysplasia in the premature infant To understand the epidemiology and physiology of bronchopulmonary dysplasia

E N D
Bronchopulmonary Dysplasia NICU Night Curriculum
Learning Objectives To understand the clinical course and presentation of bronchopulmonary dysplasia in the premature infant To understand the epidemiology and physiology of bronchopulmonary dysplasia To review the management of bronchopulmonary dysplasia
Case #1 It’s July, and you’ve just started your first month as a pediatrics intern… and you’re scheduled to start in the NICU. Someone signed out to you last night, but they were hurrying to make it in time for their “I’ll never be an intern again party” and you didn’t ask a lot of questions because you didn’t want to look dumb (already!). So you really don’t have any clue what is going on, and here is your first patient…
Case: One-liner • Baby Smith is an ex-23 wk infant, now 60 days old, who has a history of RDS, grade II IVH, and feeding intolerance, who is currently still intubated. • SO… what can you gather so far? • What is the baby’s corrected gestational age? • How bad do you think his lungs are? • What other things might you want to know from his history that would support your assessment of his lung disease?
Case: One-Liner • Baby Smith is an ex-23 wk infant, now 60 days old, who has a history of RDS, grade II IVH, and feeding intolerance, who is currently still intubated • SO… what can you gather so far? • What is the baby’s corrected gestational age? • 32 weeks • How bad do you think his lungs are? • Pretty bad • What other things might you want to know from his history that would support your assessment of his lung disease? • Maternal history, delivery, hospital course
Case: Pertinent History • Maternal history: • Mom is a 25yo G2P2 who came into L&D at 23 wks with preterm labor and rupture of membranes. • Mom did not receive antenatal steroids • Serologies: A+, RPR NR, Hep B neg, RI, HIV neg, GBS unknown • Birth history/Delivery room course: • The peds team was called to a code blue for 23 wk prematurity and precipitous delivery (she delivered 1 hour after arriving to L&D). • At delivery, the infant had a HR>100, but no respiratory effort, and was limp and blue • He required intubation and PPV and color/tone improved. • Apgars were 2 and 7. BW was 600grams. • WHAT ASPECTS OF THIS HISTORY MAKE YOU WORRY ABOUT HIS LUNGS? • His risk factors for chronic lung disease are: Prematurity, NO antenatal steroids, low birth weight
Case: NICU course • NICU course: • Respiratory: Infant was brought back to unit intubated, but was found to have a pneumothorax on admission CXR. Chest tube was placed and no other doses of surfactant were given. • Since then, infant has been intubated. Around DOL 30, extubation was attempted, but the baby had significant desaturations and increased work of breathing and was reintubated. Same story around DOL 50, but he lasted maybe a week before reintubation.
Case: At the bedside • At the bedside: • Physical exam: • Gen: You see a small baby, who is intubated. • CV:When you listen to his chest, you hear regular heart sounds and III/VI systolic murmur. • Pulm: You notice coarse breath sounds bilaterally, with occasional rales, fair chest rise with each ventilator breath and occasionally, he spontaneously takes his own breaths. • Abdom: His abdomen is soft and non-distended • Neuro: He moves his arms and legs around while you are examining him. • You look over at his ventilator and he’s on the following settings: • FiO2 55%, Pressure control 20, Pressure support 14, rate 45, I-time 0.35, PEEP 6
Case: Imaging • His chest xray today: • What do you see on this xray (Give 4 findings)?
Case: Imaging • What do you see on his xray? • ETT • Nasal Gastric Tube • Normal cardiac sillhouette • Bones look normal • GROUND GLASS APPEARANCE OF LUNGS
Blood Gas • Labs: BMP, CBC are normal. Capillary blood gas today: 7.25/65/28/+1 • What does this gas show? • RESPIRATORY ACIDOSIS
Case: Diagnosis? • Based on this baby’s history, exam, labs and xray findings, what do you think is the diagnosis? • This baby is likely developing bronchopulmonary dysplasia (or chronic lung disease) • but we will try and make some management changes during your month in the NICU to help him out. • We can then evaluate the baby at 36 weeks corrected GA (the end of your month) to see if he fits the criteria for BPD.
Bronchopulmonary Dysplasia • Most common severe complication of prematurity • First defined by Northway in 1967: lung disease resulting from prolonged mechanical ventilation in premature infants with surfactant deficiency • NICHD criteria: need for oxygen based on GA and severity of disease
Bronchopulmonary Dysplasia • “Old BPD” (before surfactant and steroids) • Cystic changes, heterogeneous aeration • “New BPD” (after surfactant and steroids) • More uniform inflation and less fibrosis, absence of small and large airway epithelial metaplasia and smooth muscle hypertophy • Some parenychmal opacities, but more homogenous aeration and less cystic areas • PATHOLOGIC HALLMARKS: larger simplified alveoli and dysmorphic pulmonary vasculature
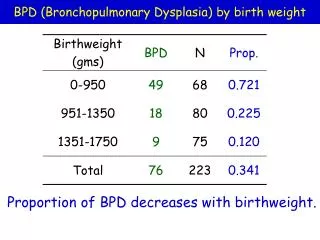
Epidemiology • Incidence: • 42-46% (BW-501-750g) • 25-33% (BW=751-1000g) • 11-14% (BW=1001=1250g) • 5-6% (BW=1251-1500g) • Risk factors: • Prematurity, low BW • White boys • Genetic heritability
Pathophysiology • Old BPD: • Airway injury, inflammation and parenchymal fibrosis due to mechanical ventilation and oxygen toxicity • New BPD: • Decreased septation and alveolar hypoplasia leading to fewer and larger alveoli, so less surface area for gas exchange • Dysregulation of vascular development leading to abnoraml distribution of alveolar capillaries and thickened muscular layer of pulmonary arterioles
Clinical Presentation Need for supplemental oxygen. Hypoxemic and hypercapneic. Exam: tachypnea, retractions, scattered rales CXR: diffusely hazy with alternating areas of atelectasis and hyperexpansion; streaky densities or cystic areas, edema CLINICAL COURSE: Tend to slowly improve and wean off respiratory support. May have intermittent episodes of acute deterioration if severe disease. May also develop pulmonary hypertension when severe
Treatment: Prevention • Prevention: • Avoidance of preterm birth • Antenatal steroids
Case: Current Management FEN: TF 150ml/kg/d of continuous NGT feeds of SSC 24 kcal. Has been gaining about 70 grams/week for the last two weeks. Resp: currently intubated at the aforementioned settings with blood gas from last slide. CV: last echo done 2 weeks ago shows a small PDA and PFO. No evidence of RVH. Heme: Hematocrit=24 checked 2 days ago Meds: multivitamin, iron, caffeine So, in practical terms, what things could you do to optimize his management over the next few weeks?
Case: Current Management • FEN: • Fluid restriction/diuretics • Optimize caloric intake and growth • Resp: • Ventilator management • Give steroids before another extubation attempt? • CV: • PDA closure? • Heme: • Transfusion to improve oxygen carrying capacity
Prognosis • Morbidity: • Higher rates of hospitalization in the first year of life e.g. resp infections • Respiratory symptoms may persist into adulthood • Abnormal pulmonary function • Asthma-like symptoms • Airway abnormalites e.g. tracheomalacia • Pulmonary artery hypertension • BPD associated with worse neurodevelopmental outcomes
Review Questions 1. What is BPD? 2. Who is at risk for developing BPD? 3. How is old and new BPD different? 4. What is the clinical course of BPD? 5. What are some methods of managing BPD? 6. What is the long-term outcomes of BPD?
Review Answers 1. What is BPD? Lung disease of premature infants, characterized by abnormal alveolarization and pulmonary vascularization. 2. What are the greatest risk factors for developing BPD? Prematurity and low birth weight 3. How is old and new BPD different? Old is before surfactant and antenatal steroids, and has more inflammation and fibrosis, whereas new BPD is post-surfactant and steroids, and shows fewer and larger alveoli.
Review Answers • 4. What is the clinical course of BPD?. Infants with BPD tend to improve slowly over time, requiring less and less respiratory support. But in severe cases, infants can have “BPD exacerbations”, require tracheostomy, or develop cor pulmonale. • 5. What are some methods of managing BPD? Fluid restriction, diuretics, optimize nutrition, permissive hypercapnea, lower goal oxygen saturations, steroids • 6. What is the long-term outcomes of BPD? Infants with BPD may have abnormal respiratory function, asthma-like symptoms, airway problems, and/or require more frequent hospitalization later in childhood. In addition, studies show that BPD is associated with worse neurodevelopmental outcomes.
References Adams et al. Pathogenesis and clinical features of bronchopulmonary dysplasia. UpToDate. May 2011. Bhandari A and Vineet Bhandari. Pitfalls, Problems, and Progress in Brocnhopulmonary Dysplasia. Pediatrics. 2009;123; 1562-1573. Fanaroff AA, et al. Trends in neonatal morbidity and mortality for very low birthweight infants. Am J Obstet Gynecol. 2007: 196(2): 147.e1-147.e8. Harris et al. Pulmonary outcomes in bronchopulmonary dysplasia. UpToDate. May 2011. Jobe Alan H. The new bronchopulmonary dysplasia. Current Opin Peds. 2011, 23: 167-172.