Download
1 / 27
280 likes | 514 Views
Bronchopulmonary Dysplasia. NICU. Definition. BPD is a clinical diagnosis, defined by oxygen dependence for a specific period of time after birth and accompanied by characteristic radiographic findings that correspond to anatomic abnormalities.

E N D
Definition • BPD is a clinical diagnosis, defined by oxygen dependence for a specific period of time after birth and accompanied by characteristic radiographic findings that correspond to anatomic abnormalities. • Northway’s definition of classic BPD in the 1960 was based on progressive radiographic changes in preterm infants who where treated for severe RDS immediately after birth and had prolonged ventilator and oxygen dependence.
This form of BPD occurred in larger relatively mature pre term infants who required treatment with high pressure ventilation and high concentrations of oxygen. Although the acute respiratory distress initially improved in these infants, oxygen requirements increased 7 to 10 days after birth and persisted for at least 28 days.
The definition of BPD was subsequently modified by Bancalari to include preterm infants who had less severe RDS that initially required short term mechanical ventilation, but who also developed persistent respiratory symptoms and oxygen requirements for at least 28 days after birth accompanied by radiographic changes.
The presentation of BPD continued to evolve with advent of antenatal steroids and postnatal surfactant, which reduced the incidence and severity of RDS and increased the survival of extremely small, very immature infants(<30 weeks gestation or<1,250g BW). These infants had milder chronic pulmonary problems that often resolved by discharge. Shennan noted that the need for supplemental oxygen until at least 36 weeks postconceptual age (PCA) in these infants was much more predictive of later pulmonary morbidity.
He therefore,recommended that oxygen dependence at 36 weeks PCA,instaed of 28 days after birth,be used as a more clincally relevant definition of BPD.
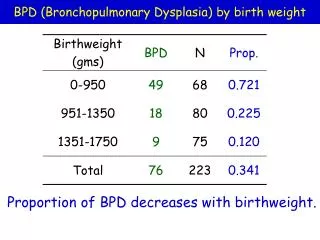
Epidemiology The risk of BPD is multifactorial. It is related directly to the severity of the initial lung disease(most often RDS) and the duration of mechanical ventilation and oxygen administration. BPD is related inversely to birthweight and gestational age ,with the smallest,sickest,most immature infants being at highest risk. The increased susceptability of the very preterm may reflect the anatomic,developmental,and reparative immaturity of the neonatal lung at the time of lung injury.
The risk of BPD is also increased by • A hemodynamically significant patent ductus arteriosus, • Postnatal sepsis, • Antenatal maternal infection(chorioamnionitis), • Maternal or neonatal colonisation with Ureaplasma histolyticum.
Term and near term infants also are at risk for BPD following severe respiratory failure treated with very high oxygen concentrations,mechanicalventilaton,and extracorporeal membrane oxygenation(ECMO). • BPD occurs in up to 27% of term or near-term infants who have very severe primary respiratory disease: • RDS,meconiumaspiration,pneumona,sepsis • In up to 50% of those who have underlying pulmonary hypoplasiae.g congenital diaphragmatic hernia,and are treated with or eligible for ECMO.
Advances in neonatal care have decreased the incidence of BPD only in the larger ,more mature preterm infants. The risk of BPD in VLBW infants is not reduced by antenatal steroids,surfactantadministration,or any specific type of respiratory support(e.g conventional ventilation or high frequency ventilation),although the disease is less severe than in the past. However ,there are substantial differences in the incidence of BPD between different centre suggesting that the overall approach to respiratory support is important.
Centers that emphsize gentle ventilation that minimise lung injury(e.g permissive hypercapnea,lower airway pressures,avoidance of intubation or early extubation) have substantially lower rates of BPD. Vitamin A ,known to protect epithelial integrity and promote normal cell differentiation and growth is associated with a small but significant decrease in the risk of BPD when administered parenterally immediately after birth.
Postnatal dexamethasone has been reported by some to decrease oxygen dependence at 36 weeks after birth,but serious short and long term complications preclude routine use. • Prevention of BPD remains elusive,ultimately depending on • avoiding or delaying premature birth, • reducing antenatal and postnatal infections,and • postanatal exposure to noxious agents,such as intubation,oxygen,and ventilation.
Pathogenesis • BPD appears to be the common path for lung injury. • Initially it was thought to be the consequence of direct trauma from mechanical ventilation and oxygen toxicity. • As the clinical presentation has changed and oxygen dependence has developed in the absence of RDS or initial oxygen exposure,inflammation has emerged as the central disease process.
Anatomic and developmental immaturity modify the lungs response to trauma amd inflammation. • Evidence of inflammatory response that accompanies RDS ,includes • Activated inflammatory cells, • inflammatory mediators,and cytokines,persist in infants who develop BPD.
Barotrauma and volutrauma from mechanical ventilation may injure airways and lung parenchyma directly and indirectly. Intubation traumatises local tissue surfaces, destroys normal ciliary action and introduces pathogens and exogenous gases directly into the airway. Air leaks further disrupt lung tissue Oxygen exposure generates toxic free radicals that cause acute tissue injury, incite inflammation, and inhibit normal repair and development.
At autopsy,infants dying of BPD have evidence of abnormal lung morphology and development,with decreased alveolarization and septation. Ultimately, BPD must be outgrown. As airways become larger,alveolarization proceeds and previously injured lung represents a smaller portion of total lung volume . Fortunately, alveolar growth continues up to 5 years of age allowing infants who have BPD to recover clinically even though Pathologic and radiologic abnormalities often persist into adulthood.
Clinical aspects • BPD results in chronic respiratory insufficiency and prolonged oxygen dependence for many weeks or months. • Clinical manifestation include tachypnea,retractions,wheezing,andrales. • Ventilation/perfusion mismatch and increased physiologic dead space result in hypercapnea and hypoxemia. • The risk of superimposed infection is increased
For all forms of BPD and CLD,oxygen requirements begin to increase at the end of the first week after birth,reaching a stable plateau by the beginning of the third week. • Clinical exercabations occur in association with • Pulmonary edema, • Superimposed infection, • or right heart failure.
Bronchospasm,episodes of cyanosis,and chronic hypoxemia often accompany BPD. • Early pulmonary function abnormalities in infants who have BPD include decreased lung compliance,ventilation perfusion mismatch,and increased lung volume,airway resistance and air trapping
Clinical improvement in BPD is heralded by improvement in somatic growth. • Infants who develop BPD are at increased risk of • patent ductus arteriosus, • sepsis, • intraventricular hemorrhage(IVH), • retinopathy of prematurity,and death.
Management • The treatment goals of BPD focus on • relieving respiratory symptoms, • improving lung function, • minimizing ongoing lung injury, • reducing inflammation, • maintaining adequate oxygenation, and • facilitating lung growth.