Download
1 / 33
330 likes | 500 Views
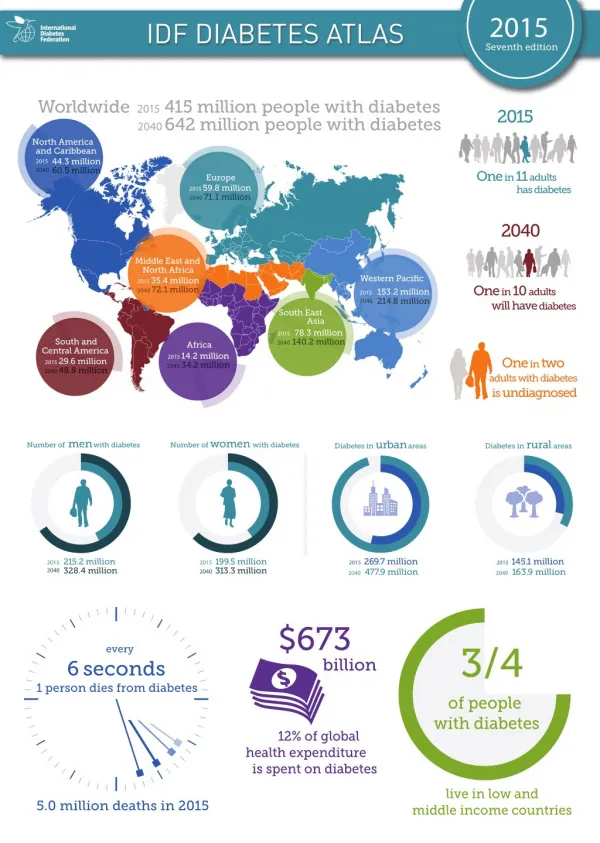
Acute Diabetes Case Study E. Ainsley McDonald Veronica Nou Poonam Shrestha Mary Tormey. What is Lactic Acidosis?. What is Lactate. Formed from: Pyruvate + NADH + H + <-> Lactate + NAD + All tissues produce lactate under anaerobic conditions.

E N D
Acute Diabetes Case Study E Ainsley McDonald Veronica Nou Poonam Shrestha Mary Tormey
What is Lactate • Formed from: Pyruvate + NADH + H+ <-> Lactate + NAD+ • All tissues produce lactate under anaerobic conditions.
Lactate is metabolised predominately in the liver (60%) and kidney (30%). • Half is converted to glucose and half is further metabolised to C02 and water in the citric acid cycle.
Mechanisms involved in Lactic Acidosis • Lactic Acidosis is due to: • Excessive tissue lactate production • Impaired hepatic metabolism of lactate • In most cases both processes are often contributing.
Definitions • Hyperlactaemia: a level from 2 mmols/L to 5 mmol/L • Severe Lactic Acidosis: when levels are greater than 5 mmols/L • Acidosis: Arterial Blood pH of less than 7.35 with a plasma bicarbonate concentration of less than 22 mmol/L
Types of Lactic Acidosis • Type A: - Tissue oxygen delivery is inadequate. • Inadequate 02 -> slowing of mitochrondrial metabolism -> pyruvate is converted into lactate. Anaerobic Metabolism
Types of Lactic Acidosis Ctd. • Type B: - No clinical evidence of a reduction in tissue oxygen perfusion. - Carbohydrate metabolism is disordered and excess lactic acid is produced.
Sub- Categories of B • Type B1: Associated with underlying diseases eg. Ketoacidosis • Type B2: Associated with drugs and toxins eg. Phenformin and Biguanide hypoglycaemic • Type B3: Inborn errors of metabolism eg. Congentital enzyme defects (Pyruvate dehydrogenase deficiency.)
Signs and Symptoms of Lactic Acidosis • Initially: - Nausea, vomiting, bloating, abdominal pain and lack of appetite, difficulty breathing and diarrhea. • Other signs include: - Hepatomegaly, Elevated Liver enzymes, low bicarbonate, raised lactate and deteriorating kidney function.
Mary’s History • 70 years of age, 60kg, BMI of 22kg/m2 • Serum creatinine of 0.15mmol/L (normal range 0.05-0.12mmol/L) • Creatinine Clearance = [(140-age)*weight]/815*serum creatinine = 34mmol/L • Medications include: gliclazide 160mg BD, metformin 850mg TDS, glyceryl trinitrate 600mcg PRN, simvastatin 40mg N
Stable angina for previous 10 months following MI • Angioplasty for occluded right coronary artery • Diffuse coronary artery disease not amenable to angioplasty or bypass grafting • Diabetes (well controlled) – microvascular complications include stable background diabetic retinopathy, minor renal impairment, and reduced peripheral sensation • Admitted to A&E with severe chest pain – died 10 hours later from lactic acidosis complicating MI. • So why lactic acidosis?
Mary’s Medications • Metformin 850mg TDS – • Biguanide indicated for Type 2 Diabetes. • Max recommended dose, (max dose 3g). • Metformin accumulation causes the rare adverse effect of lactic acidosis WHICH IS OFTEN FATAL. • Should be replaced with insulin if possible in cases of renal impairment • Contraindicated when creatinine clearance less than 50mL/min as there is a risk of lactic acidosis.
Mary’s Medications • Gliclazide 160mg BD – sulfonylurea indicated for Type 2 Diabetes. On max dose. • Simvastatin 40mg N – rare adverse effects include hepatitis and liver failure, the risk of which is increased by pre-existing liver function abnormalities. Liver function should be monitored before starting treatment, at 3 months and then at 6 month intervals. • Glyceryl Trinitrate 600mcg PRN – for treatment of acute angina. BUT there seems to be no long acting nitrate for prevention of anginal attacks.
Management of Lactic Acidosis • Generally supportive • Isolate cause of increased lactate production or decreased lactate clearance and treat • Sodium bicarbonate (NaHCO3) used to treat acid base disturbance • Role controversial as treats only acidaemia and not underlying cause, and use may result in sodium and fluid overload, hypokalaemia, CNS acidosis, hypercapnia, and alkalosis as a result of overshoot. • NaHCO3 required (mEq) = [(HCO3-)desired – (HCO3-)observed * 0.4 * body weight (kg)]
If patient renally insufficient or there is a threat of hypervolaemia, the Merck Manual 2000 recommends hemofiltration or hemodialysis. • Another proposed alternative is the use of dichloroacetate, as it enhances the oxidation of lactic acid, but clinical trials so far have shown little benefit.
Clinical chemistry test for Myocardial Infarction • Cardiac Enzyme in the blood
Cardiac Markers • Most conclusive evidence for infraction is an increase in CARDIAC ENZYMES • Specific patterns of enzyme release are sensitive and specific markers for acute MI • Cardiac Markers -aspartate transaminase(AST) -Lactate dehydrogenase(LDH) -creatinine kinase (CK) - troponin
CK, CK-MB and CK-MB index • Creatinine Kinase(CK) -rises 4 to 6 hours after M.I., peaks at 12 to 24 hours and returns to normal by 3 to 4 days • CK-MB is more specific than total CK • CK-MB index is only calculated when CK-MB is elevated -CK-MB index >2.5cardiac damage
Lactase dehydrogenase • Specific to heart and changes during MI • Rise above the reference range within 24 hours of an AMI • Reaches the peak within 3-6 days • Returns to baseline within 8-12 days
Troponin in AMI • Troponin level will rise at the same time as CK,CK-MB but continues to rise for a longer periods. • Troponin would have risen 4 to 6 hours after M.I., and its level remains elevated for 14 days. • They are very specific for cardiac muscle, not elevated with skeletal muscle damage or in renal failure as with CK and CK-MB.
Lactic acidosis • A lactate concentration of 5 mEq/L or greater & arterial pH of 7.35 or less identify significant lactic acidosis • Although by definition: a lactate level greater than 2, levels of 2-5 represent gray areas & are of questionable clinical significance (Mizock, 2001, 1997)
Lactic acidosis • Lactate levels of > 5 mM have been associated with 30 day mortality of 83% USA study 1994 • the higher the blood lactate level the worse the prognosis, survival is unlikely at levels >25 • If the level falls 5-10% within an hour of starting resus - prognosis is fairly good
? Lactic acidosis in the diabetic • Most diabetics with lactic acidosis are in shock or have severe underlying disorders associated with the syndrome Mizock 1992 1989 • Usually present with ketoacidosis • The incidence of lactic acidosis in patients with ketoacidosis is low - probably < 10% Strangaard 1971 • Lactate is not elevated well in controlled diabetics unless they are acutely ill Mizock 1989 1992
Lactic acidosis -ABGs • Acidosis metabolic- caused by the generation of lactic acid, pCO2 is subnormal if respiratory compensation occurs & pH varies from normal to significantly lowered (guide < 7.35) • Alkalosis respiratory- there is an antecedent or coexistent respiratory alkalosis in many conditions associated with LD- a mixed AB disorder is frequently present
LA-ABGs • Acute hypoxia is associated with an MI • When arterial pO2 was 26-32 mmHg lactate rose 3-4 mmol/L Huckabee 1958 • However: • Hyperlacteamia. Is nota reliable indicator of tissue perfusion or O2 debt because multiple mechanisms contribute to the lactate level eg hypoxia, ^aerobic metabolism, endotoxins & catecholamines
LA or DKA or both? • Hyperglyceamia not associated with LA but with DKA • Ketonuria strongly associated with DKA • Hyperosmolality is associated with DKA • Suspect LA if level of anion gap high & ketonuria low
BUN • RF is frequently associated with LA either in Type a due to poor tissue perfusion or type b for which the MOA is unclear
Measuring anion gap • Na - (Cl + HCO3-) • normal was 12 +/- 4 mEq/L • now due to new techniques of measurement in labs, normal has decreased may be as low as 5 to 12 Merck manual p157 17th ed
Anion gap - increased in lactic acidosis • The decrease in bicarbonate is approximately equal to the increase in the anion gap • It may be an unreliable indicator of LA because of hyperchloreamia by N/S IVIs, hypoalbuminemia, & mixed AB disorders • 0.25 x normal - observed albumin + AG = adjusted AG in presence of hypoalbuminemia
Other serum levels which may be seen with LA • phosphate • + in tissue hypoxia with shock • lower levels- associated with DKA • Calcium • low Ca possibly due to chelation of free calcium by lactate ions or admin of sodium bicarbonate • Uric acid high competes with lactate for excretion
potassium • Increased in severe acidosis because hydrogen cations enter cells and K ions exit to maintain neutrality, also often due to renal failure • Normal serum K - may be due to H & lactate moving into cells together & so not requiring r/o cation out of cell
LFTs • The liver is the main route for lactate disposal by gluconeogenesis or oxidation of lactate • In acidosis gluconeogenesis in the liver is decreased so lactate accumulates • at pH < 7.0 the liver will actually generate lactate.