Download
1 / 31
310 likes | 315 Views
A collation of pre-clinical and phased trial data on the Epigenetic Reprogramming Technology injections offered by Moderna Inc.

E N D
SARS-CoV-2 mRNA Vaccine Development Enabled by Prototype Pathogen Preparedness (which was not certified by peer review) – June 11, 2020 performedon Mice (39 pages) Here, we show that mRNA-1273 induces both potent neutralizing antibody and CD8 T cell responses and protects against SARS-CoV-2 infection in lungs and nosesof micewithout evidence of immunopathology. mRNA-1273is currently in a Phase 2 clinical trial with a trajectory towards Phase 3 efficacy evaluation. As part of our pandemic preparedness efforts, we have studied MERS-CoV as prototype pathogen forbetacoronavirusesto optimize vaccine design, to dissect the humoral immune response to vaccination, and identify mechanisms and correlates of protection. Within 5 days of sequence release, current Good Manufacturing Practice (cGMP) production of mRNA/LNP expressing the SARS-CoV-2 S-2P as a transmembrane-anchored protein with the native furin cleavage site(mRNA-1273) was initiated in parallel with preclinical evaluation. Remarkably, this led to the start of a first in human Phase 1 clinical trial on March 16, 2020, 66 days after the viral sequence was released (January10/11), and a Phase 2began 74 days later on May 29, 2020 Immunogenicity was assessed in six-week old female BALB/cJ, C57BL/6J, and B6C3F1/J mice by immunizing intramuscularly (IM) twice with 0.01, 0.1, or 1 μg of mRNA-1273 at a 3-week interval. mRNA-1273 induced dose-dependent S-specific binding antibodies after primeand boostin all mouse strains
Also Known As: C, BALBc BALB/cJ(6-8-week-old females in this study) is a commonly used inbred. Key traits include a susceptibility to developing the demyelinating disease upon infection with Theiler's murine encephalomyelitis virus. The BALB/cJsubstrain is susceptible to Listeria monocytogenes, all species of Leishmania, and several species of Trypanosoma, but is resistant to experimental allergic orchitis(EAO) C57BL/6Jmice are used in a wide variety of research areas including cardiovascular biology, developmental biology, diabetes and obesity, genetics, immunology, neurobiology, and sensorineuralresearch. C57BL/6Jmice are also commonly used in the production of transgenic mice. Overall, C57BL/6J mice breed well, are long-lived, and have a low susceptibility to tumors. Primitive hematopoietic stem cells from C57BL/6J mice show greatly delayed senescence relative to BALB/c and DBA/2J. Other characteristics include: 1) a high susceptibility to diet-induced obesity, type 2 diabetes, and atherosclerosis; 2) a high incidence of microphthalmia and other associated eye abnormalities; 3) resistance to audiogenic seizures; 4) low bone density; 5) hereditary hydrocephalus (early reports indicate 1 - 4 %); 6) portosystemic shunts(~5%); 7) hair loss associated with overgrooming; 8) a preference for alcohol and morphine; 9)
Next, we evaluated the balance of Th1and Th2, because vaccine associated enhanced respiratory disease (VAERD) has been associated with Th2-biased immune responses in children immunized with whole-inactivated virus vaccines against RSV and measles virus [25,26.] Thus, we first compared levels of S-specificIgG2a/cand IgG1, which are surrogates of Th1 and Th2 responsesrespectively, elicited by mRNA-1273 to those elicited by SARS-CoV-2 S-2P protein adjuvantedwith the TLR4-agonistSigma Adjuvant System (SAS). Following re-stimulation with peptide pools (S1 and S2) corresponding to the S protein, splenocytesfrom mRNA-1273-immunized mice secreted more IFN-γthan IL-4, IL-5, or IL-13 whereas SARS-CoV-2 S protein with alum (Hydrogel) induced Th2-skewed cytokine secretion 7 weeks post-boost, we also directly measured cytokine patterns in vaccine-induced memory T cells by intracellular cytokine staining (ICS); mRNA-1273-elicitedCD4+ T cells re-stimulated with S1 or S2 peptide pools exhibited a Th1-dominant response, particularly at higher immunogendoses. Furthermore, 1 μg of mRNA-1273 induced a robust CD8+ T cell response to the S1 peptide pool Protective immunity was assessed in young adult BALB/cJmicechallenged with mouse adapted (MA) SARS-CoV-2 that exhibits viral replication localized to lungs and nasal turbinates[28]. In summary, mRNA-1273 is immunogenic, efficacious, and does not show evidence of promoting VAERD when given at sub-protective dosesin mice. A major goal of animal studies to support SARS-CoV-2 vaccine candidates through clinical trials is to not only prove elicitation of potent protective immune responses, but to show that sub-protective responses do not cause VAERD[3]
These data, combined with immunogenicity data from nonhuman primates and subjects in early Phase 1 clinical trials, will be used to inform the dose and regimen of mRNA-1273 in advanced clinical efficacy trials. This is a demonstration of how the power of new technology-driven concepts like synthetic vaccinologyfacilitate a vaccine development program that can be initiated with pathogen sequences alone [11] We thank members of the NIH NIAID VRC Translational Research Program for technical assistance with mouse experiments. This work was supported by the Intramural Research Program of the VRC and the Division of Intramural Research, NIAID, NIH(B.S.G) and NIH NIAID grant R01-AI127521 (J.S.M.). mRNA-1273 has been funded in part with Federal funds from the Department of Health and Human Services, Office of the Assistant Secretary for Preparedness and Response, Biomedical Advanced Research and DevelopmentAuthority, under Contract75A50120C00034 To produce SARS-CoV-2 pseudoviruses, a codon-optimized CMV/R-SARS-CoV-2 S (clinical isolate 2019-nCoV/USA-WA1-F6/2020Wuhan-1, Genbank #: MN908947.3) plasmid was constructed. Pseudoviruses were produced by co-transfection of plasmids encoding a luciferase reporter, lentivirus backbone, and S genes into HEK293T/17 cells(ATCC #CRL-11268), as previously described [33]. For SARS-CoV-2 pseudovirus, human transmembrane protease serine 2 (TMPRSS2) plasmidwas also co-transfected [34] Note: International Patent Application No. WO/2018/081318 entitled “Prefusion Coronavirus Spike Proteins and Their Use.” and US Patent Application No. 62/972,886 228 entitled “2019-nCoV Vaccine”.
MERS-CoV and SARS-CoV Protein Expression and Purification Vectors encoding MERS-CoV S-2P11 and SARS-CoV S-2P22were generated as previously described with the following small amendments. Proteins were expressed by transfectionof plasmids into 1Expi293 cells using Expifectamine transfection reagent (1ThermoFisher). The rabbit IgG that is produced in Expi293F™ cells after transfection with the control vector is secreted into the Expi293. Expi293™ Expression System is a high-yield transient expression system based on suspension-adapted Human Embryonic Kidney (HEK-293) cells(See next slide for data) For proteins used for mouse inoculations, tags were cleaved with addition of HRV3C protease(ThermoFisher). Alternative names: Human Rhinovirus 3C • Source: Escherichia coli (E.coli) 2Thermo Scientific Pierce Human Rhinovirus (HRV) 3C Protease is a recombinant cysteine protease used to remove fusion tags from proteins with the HRV 3C cleavage sequence and is dual tagged for easy removal from the sample after cleavage. 3HEK293T/17(ATCC #CRL-11268), VeroE6(ATCC), Huh7.5 cells (provided by Deborah R. Taylor, US Food and Drug Administration), and ACE-2-expressing 293T cells (provided by Michael Farzan, Scripps Research Institute) 1 https://assets.thermofisher.com/TFS-assets /LSG/manuals/MAN0019402_Expi293_ExpressionSystem_3L_UG.pdf 2 https://www.thermofisher.com/order/catalog/product/88946#/88946 3 https://www.lgcstandards-atcc.org/products/all/CRL-11268.aspx?geo_country=gb
Twenty-five days after viral sequences were released, clinically-relevant mRNA-1273was received to initiate animal experiments. Immunogenicity in micewas confirmed 15 days later. Moderna shipped clinical drug product 41 days after GMP production began, leading to the Phase 1 clinical trial starting 66 days following the release of nCoVsequences.
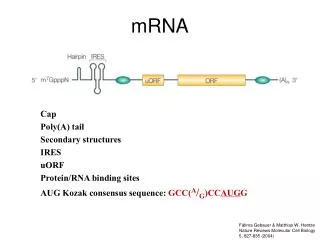
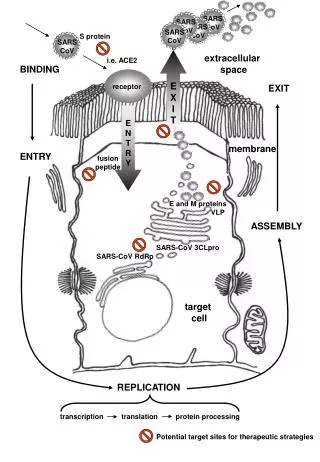
aCurrent status of SARS-CoV-2 Vaccine candidates (Over 165 currently in development) 32 are conducting in-human trials Synbiobeta, the network of the synthetic biology world - Genetic Vaccines Moderna– Phase 3 trial, July 27 - Moderna, the biotech with the most advanced mRNA COVID-19 vaccine, selected100 µg as the dose for its phase 3 clinical trial (see later slides). mRNA-1273 COVID-19 vaccine Sponsors: NIH, DARPA, Vaccine Research Center (VRC) of NIAID for MERS-CoV 9along with NIH), and CEPI The governmenthas bankrolled Moderna’sefforts on a coronavirus vaccine with nearly $1 billion. On August 11, the government awarded the company an additional $1.5 billion in exchange for 100 million dosesif the vaccine proves safe and effective. StéphaneBancel, Moderna’sCEO: “vaccines normally take 10 years to make.” Target: Spike (S) protein (via Lymph Nodes according to promotional video) complexis necessary for membrane fusion andhost cell infectionandinduction of Th-1 biased, CD4+ T-cells (SeeAdenovirus) All of the uridinesin Moderna’s mRNAs are modified to evade the normal immune response triggered when toll life receptors—specifically TLR7 and TLR8—recognizeuridineand activate an interferon response Special Note: June 17, 2020 - Reuters reported Israel has signed an agreement with Modernafor the future purchase of its potential COVID-19 vaccine. ahttps://www.nytimes.com/interactive/2020/science/coronavirus-vaccine-tracker.html (updated August 21, 2020
Moderna - mRNA vaccine against SARS-CoV-2 (mRNA-1273) When the company received the SARS-CoV-2 genomic sequences from China on January 11, the stage was already set. RNA is a great molecule to hitch a wagon to, Bancel noted, as it has many dimensions to play with. All of the uridinesin Moderna’s mRNAs are modified to evadethe normal immune response triggered when toll life receptors - specifically TLR7and TLR8 - recognize uridine and activate an interferon response. One of the reasons the SARS-CoV-2 vaccine development has been so fast is the work Moderna has done over the past two years in an existing collaboration with the Vaccine Research Center (VRC) of NIAID to develop a vaccine against MERS-CoV. March 2, FDAgave the green light to start clinical study. The first person was dosed last Monday and the company is currently filing an IND to start Phase II.
Actual Study Start Date: March 16, 2020 Estimated Primary Completion Date: November 22, 2021 Estimated Study Completion Date: November 22, 2021 120 participants Phase I, Open-Label, Dose-Ranging Study of the Safety and Immunogenicity of 2019-nCoV Vaccine (mRNA-1273) in Healthy Adults
AnmRNA Vaccine againstSARS-CoV-2 - Preliminary Report, July 14, 2020 Funded by the National Institute of Allergy and Infectious Diseases and others; mRNA-1273 ClinicalTrials.gov number, NCT04283461. We conducted a phase 1, dose-escalation, open-label trial including 45 healthy adults, 18 to 55 years of age, who received two vaccinations, 28 days apart, with mRNA-1273 in a dose of 25 μg, 100 μg, or 250 μg. There were 15 participants in each dose group Solicited adverse events that occurred in more than half the participants included fatigue, chills, headache, myalgia, and pain at the injection site. Systemic adverse events were more common after the second vaccination, particularly with the highest dose, and three participants (21%) in the 250-μgdose groupreported one or more severe adverse events. The candidate vaccine mRNA-1273 is a lipid nanoparticle–encapsulated, nucleoside-modified messenger RNA (mRNA)–based vaccine that encodes the SARS-CoV-2 spike (S) glycoprotein stabilized in its prefusion conformation. The S glycoprotein mediates host cell attachment and is required for viral entry [3]; it is the primary vaccine target for many candidate SARS-CoV-2 vaccines [4-7]. The 45 enrolled participants received their first vaccination between March 16 and April 14, 2020. Three participants did not receive the second vaccination, including one in the 25-μg group who had urticaria on both legs,with onset 5 days after the first vaccination(transienturticaria, judged to be related to the first vaccination). Solicited systemic adverse events were more common after the second vaccination and occurred in 7 of 13 participants (54%) in the 25-μg group, all 15in the 100-μg group, and all 14 in the 250-μg group, with 3 of those participants (21%) reporting one or more severe events.
SARS-CoV-2 T-Cell Responses The 25-μg and 100-μg doses elicited CD4 T-cell responsesthat on stimulation by S-specific peptide pools were strongly biased toward expression of Th1 cytokines (tumor necrosis factor α> interleukin 2 > interferonγ), with minimal type 2 helper T-cell (Th2) cytokine expression (interleukin 4 and interleukin 13). CD8 T-cell responses to S-2P were detected at low levels after the second vaccination in the 100-μg dose group. Greater reactogenicity followed the second vaccination, particularly in the 250-μg group. This descriptive safety profile is similar to that described in a report of two trials of avian influenza mRNA vaccines(influenza A/H10N8 and influenza A/H7N9) that were manufactured by Moderna with the use of an earlier lipid nanoparticle capsule formulation[11] and is consistent with an interim report of a phase 1–2 evaluation of a Covid-19 mRNA vaccine encoding the S receptor-binding domain[6]. Those studies showed that solicited systemic adverse events tended to be more frequent and more severe with higher doses and after the second vaccination. In humans, phase 3 efficacy trials will allow assessment of the correlation of vaccine-inducedimmuneresponses with clinical protection. In this interim report of follow-up of participants through day 57, we were not able to assess the durability of the immune responses; however, participants will be followed for 1 year after the second vaccinationwith scheduled blood collections throughout that period to characterize the humoraland cellular immunologic responses. This longitudinal assessment is relevant given that natural history studies suggest that SARS-CoVand MERS-CoV (Middle East respiratory syndrome coronavirus) infections, particularly mild illnesses, may not generate long-lived antibody responses [20-22]
These features of the mRNA composition and formulation have been associated with prolonged protein expression, induction of antigen-specific T-follicular helper cells, and activation of germinal center B cells [24]. Previous experience with veterinary coronavirus vaccines and animal models of SARS-CoV and MERS-CoV infection have raised safety concerns about the potential for vaccine-associated enhanced respiratory disease. These eventswere associated either with macrophage-tropic coronaviruses susceptible to antibody-dependent enhancement (ADE) of replication or with vaccine antigensthat induced antibodies with poor neutralizing activity and Th2-biased responses [31]. Studies of mRNA-1273 in mice show that the structurally defined spike antigen induces robust neutralizing activity and that the gene-based delivery promotes Th1-biased responses, including CD8 T cells that protect against virus replication in lung and nose without evidence of immunopathology [32] These safety and immunogenicity findings supportadvancementof the mRNA-1273 vaccine to later-stage clinical trials. Of the three doses evaluated, the 100-μg dose elicits high neutralization responsesand Th1-skewed CD4 T cell responses, coupled with a reactogenicity profile that is more favourable than that of the higher dose. A phase 2 trial of mRNA-1273 in 600 healthy adults, evaluating doses of 50 μg and 100 μg, is ongoing (ClinicalTrials.gov number, NCT04405076). A large phase 3 efficacy trial, expected to evaluate a 100-μg dose, is anticipated to begin during the summer of 2020. The National Institute of Allergy and Infectious Diseases (NIAID) ultimately made all decisions regarding trial design and implementation. Funding for the manufacture of mRNA-1273 phase 1 material was provided by the Coalition for Epidemic Preparedness Innovation (CEPI). Michael Farzanfor providing the ACE2-overexpressing 293 cells;
Phase I Safety and Immunogenicity Study of 2019-nCoV Vaccine (mRNA-1273) for Prophylaxis of SARS-CoV-2Infection(COVID-19) - ClinicalTrials.gov Identifier: NCT04283461 155 (120) participants 18 years and older (no control) Subjects will receive an intramuscular (IM) injection (0.5 milliliters[mL]) of mRNA-1273on Days 1 and 29 (28 days apart) in the deltoidmuscle and will be followed through 12 monthspost second vaccination (Day 394). 10 micrograms [mcg], 25 mcg, 50 mcg, 100 mcg, and 250 mcg. 2-dose vaccination schedule
Actual Study Start Date : May 29, 2020 Estimated Primary Completion Date: March 2021 Estimated Study Completion Date: August 2021 600 participants Experimental: mRNA-1273: Dose 50 mcg &100 mcg - Adults Aged 18-54 Phase 2a, Randomized, Observer-Blind, Placebo Controlled
Study: Evaluation of the mRNA-1273 Vaccine against SARS-CoV-2in Nonhuman Primates July 28, 2020, and updated on August 7, 2020 Nonhuman primates received 10 or 100 μg of mRNA-1273, a vaccine encoding the prefusion-stabilized spike protein of SARS-CoV-2, or no vaccine. Antibody and T-cell responses were assessed before upper- and lower-airway challenge with SARS-CoV-2. Vaccinationinducedtype 1 helper T-cell (Th1)–biased CD4 T-cell responses and lowor undetectable Th2 or CD8 T-cell responses. The majority of vaccine candidates have focused on inducingantibody responses against the trimericSARS-CoV-2 spike (S) protein, a class I fusion protein that facilitates binding to the angiotensin- converting–enzyme 2 (ACE2) receptor and triggers virus–cell-membrane fusion[3] A variety of vaccine approaches [4] and formulationsfor targetingthe SARS-CoV-2 S protein are being pursued, including nucleic acid vaccines (RNA and DNA) [5-8] human and simian replication-defective adenoviral vaccines [9,10] whole-inactivated SARSCoV-2 [11,12] and subunit protein vaccines [13]. RNA vaccines encoding viral antigens have been shown to be safe and immunogenic in several clinical trials [5,15] including in a recent phase 1 clinical trial of mRNA-1273, a SARS-CoV-2 vaccine candidate [16] Data from a mouse model showing that a low dose of mRNA-1273 induced a robust neutralizing antibody response and high-level protection against SARS-CoV-2[6] raised the possibility that vaccinationwith mRNA-1273 could prevent or limit both upper- and lower-airway infectionin nonhuman primates. Female and male Indian-origin rhesus macaques (12 of each sex; age range, 3 to 6 years)
Animals were vaccinated intramuscularly at week0 and at week 4 with either 10 or 100 μg of mRNA-1273 in 1 ml of 1× phosphate-buffered saline (PBS) into the right hind leg. At week 8 (4 weeks after the second vaccination), all animals were challengedwith a total doseof 7.6×105 plaque-forming units (PFU). The stock of 1.9×105 PFU per milliliterSARS-CoV-2 (USAWA1/2020 strain) was administered in a volume of 3 ml by the intratracheal route and in a volume of 1 ml by the intranasal route (0.5 ml per nostril). SARS-CoV-2–specificT-cell immunity may have a role in pathogenesis or protection against SARSCoV-2and can influence the humoral immune response [34-36]. Activated CD4 T cells are critical for B-cell activation and antibody production and can be segregated into functional subsets on the basis of their production of specific cytokines. The inductionof CD4 type 2 helper T-cell (Th2) (interleukin-4, -5, or -13) responseshas been associated with vaccine-associated enhanced respiratory disease(VAERD), as seen in some patients withrespiratory virus infections, such as respiratory syncytial virus infection and measles[19,20] as well as in animal models of Middle East respiratory syndrome coronavirus (MERS-CoV) [21] VAERD is generally not observed when a CD4 Th1 (interferon-γ, interleukin-2, tumor necrosis factor α) response occurs in the absence of a Th2 response[35,37-39] Th1 response levels were higher in the 100-μg dose group than in the control group or in the 10-μg dose group. Even at the 10-μg dose, Th1 responses were higher than in the control group. In contrast, Th2 responses were low to undetectable in both vaccine dose groups. CD8 T-cell responses were also low to undetectableafter mRNA-1273 vaccination.
We extended the analysis of CD4 T-cell responses, given their importance in regulating antibodyresponses. CD40L is a cell-surface marker expressed after CD4 T-cell activation that mediates B-cell activation for efficient isotype switching; three of eight animals in the 10-μg dose group and seven of seven animals in the 100-μg dose group had S-specific CD40L+ CD4 T-cell responses, and 100 μg of mRNA-1273 induced greater responses than the PBS control. Since nucleoside-modified RNA vaccines encoding various viral antigens have been shown to induce robust antibody responses in nonhuman primates in association with increased CD4 T follicular helper (Tfh) cells[40] we measured interleukin-21, the canonical cytokine produced by Tfh cells. Tfh cells are critical for the formation of germinal centers and generation of longterm B-cell memory. Four of eight animals in the 10-μg dose group and seven of seven animals in the 100-μg dose group had interleukin-21 responses; the responses differed between the 100-μg dose group and the control and 10-μg dose groups, as well as between the 10-μg dose group and the control group. These data show that mRNA-1273 induced Th1 and interleukin-21–producing Tfh-cell responses. We did not find evidence of Th2 or CD8 T-cell responses in this study. Questions: Do the vaccinesinducea Th1 response including IL-2R and production of Regulatory T cells (Tregs) via CD4+ cells and are any other interleukinsbeing released (IL-6, IL-8, IL-10) The vaccine may ‘protect’ the upper and lower airways, but would it not alleviate the nasal culture or viral load from sneezing, should a ‘sneezyvirus’ be able to transmit infection by this (aerosolised) route?
Previous vaccine studies in nonhuman primates with recombinant chimpanzee-derived adenovirus vector vaccine from Oxford (ChAdOX) or DNA vaccine showed protection against lower-airway viral replication and against pathologic changes in the lung after challenge with approximately 106TCID50 (for the ChAdOX vaccine) [10] or 104 PFU (for the DNA vaccine) [7] of SARS-CoV-2. However, these studies provided no evidence of a reduction of viral replication in nasal tissue, raising questions as to whether these vaccines could affect virus transmission. On the basis of recent data in humans that show a reduction in antibodies over time [44,45] vaccine-inducedimmunitythat exceeds the antibody response to primary infection may be needed for durable protection. Studies are now under way to determine the durability of immunity and protection over 1 year after vaccination. In our study, it was notable that mRNA-1273inducedS-specific CD4 T cells that produce interleukin-21, the canonical cytokine that defines Tfh cell responses, which suggests this as an additional mechanism for generating potent antibody responses. A major potential concern in SARS-CoV-2 vaccine development is VAERD, which is associated with induction of non-neutralizing antibodies that can lead to immune complex formation, complement activation, Th2-biased responses, and immunopathologic complications. Supported by the Intramural Research Program of the Vaccine Research Center (VRC), NationalInstitute of Allergy and Infectious Diseases (NIAID), National Institutes of Health (NIH); and the Office of the Assistant Secretary for Preparedness and Response, Biomedical Advanced Research and Development Authority, Department of Health and Human Services
Modernais leading the trial as the regulatory sponsor and is providing the investigational vaccine for the trial. The Biomedical Advanced Research and Development Authority (BARDA) of the U.S. Department of Health and Human Services’ Office of the Assistant Secretary for Preparedness and Response and NIAIDare providing funding support for the trial. The vaccine efficacy trial is the first to be implemented under Operation Warp Speed, a multi-agency collaboration led by HHS that aims to accelerate the development, manufacturing and distribution of medical countermeasures for COVID-19. “Thanks to President Trump’s leadership and the hard work of American scientists, the investigational vaccine developed by NIH and Modernahas reached this Phase 3 trial at record pace,” said HHS Secretary Alex Azar. “Operation Warp Speed is supporting a portfolio of vaccines like the NIH/Moderna candidate so that, if the results of clinical trialsmeet FDA’s gold standard, these 1productscan reach Americans without a day’s delay.” 1 https://www.coronaviruspreventionnetwork.org
Phase 3: Actual Study Start Date : July 27, 2020 Estimated Primary Completion Date: October 27, 2022 Estimated Study Completion Date: October 27, 2022 30,000 participants Intramuscular(IM) injection of 100 microgram (ug) mRNA-1273on Day 1(dose 1) and on Day 29 (dose 2) (up to Day 759 (2 years after dose 2)
https://www.coronaviruspreventionnetwork.org/understanding-clinical-studies/https://www.coronaviruspreventionnetwork.org/understanding-clinical-studies/