Download
1 / 58
970 likes | 2.78k Views
Enamel . Dr. Fatma Elturki. Objectives. What is the enamel ? Physical characteristics. Chemical characteristics. Amelogenesis. Histological structure of enamel. SURFACE STRUCTURES of enamel. Age changes of enamel. Clinical considerations. Enamel .

E N D
Enamel Dr. Fatma Elturki
Objectives • What is the enamel ? • Physical characteristics. • Chemical characteristics. • Amelogenesis. • Histological structure of enamel. • SURFACE STRUCTURES of enamel. • Age changes of enamel. • Clinical considerations.
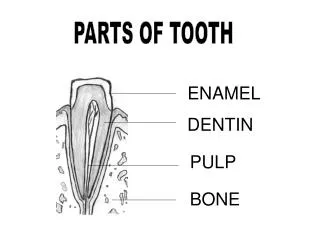
Enamel • Enamel is the most highly calcified and hardest tissue in the human body. • It cover the anatomical crown of the teeth. • It forms a protective covering of the teeth to resist the stress during mastication. • Unlike dentin, cementum and bone, enamel is produced by cells of ectodermal origin.
Physical characteristics Thickness:- the enamel thickness is variable over the entire surface of the crown Maximum thickness of about 2- 2.5 mm on the cusps. Minimum thickness at the bottom of sulcus and at cervical margin of the root. Hardness:- the enamel is considered as the hardest calcified tissue in the human body.
Physical characteristics of enamel Brittleness:- The specific structure and hardness of the enamel render it brittle. Color:- The color of enamel ranges from yellow to shades of gray or gray- blue. Permeability:- It is semipermeable, decreased by age.
Chemical characteristics of enamel • Mature enamel is made up to approximately 96% inorganic material, 1% organic material, and 3% water by weight. • The inorganic content is consists of crystalline calcium phosphate in the form of hydroxyapatite.
Amelogenesis • Amelogenesis has six phases but generally is subdividing into three main functional stages referred to as the presecretory, secretory and maturation stages. • The six phases are: • Morphogenetic. • Organizing(differentiation). • Secretory (formative). • Maturative. • Protective. • Desmolytic. Morphodifferentiation differentiation 3. Secretory (initial) 4. Secretory (Tomes’ process) Maturation (ruffle-ended) Maturation (smooth-ended) Protective
pre secretory stage • It includes: • Morphogenetic phases. • Differentiation phases.
Morphogenetic phases • Before the ameloblasts are fully differentiated, they interact with the adjacent mesenchymal cells determining the shape of the A.D.J, and the crown. During this stage the cells are short columnar with large oval nuclei that almost fill the cell body. The Golgi apparatus and centrioles are located at the proximal (basal) end of the cell facing the stratum intermedium, where as the mitochondria are evenly dispersed throughout the cytoplasm.
Differentiation phases • As the cells of the inner enamel epithelium differentiate into ameloblasts, they elongate and their nuclei shift proximally toward the stratum intermedium. • The formation of dentin by the odontoblasts begins by the end of the differentiation phase. The basement membrane supporting the preameloblasts disintegrates after the deposition of dentin and during the differentiation of ameloblasts.
Secretory stage • The cells of ameloblasts develop blunt processes which penetrate the basal lamina and protrude into the Predentin thus the basement membrane is Fragmented. • During enamel formation, the cell organelles of ameloblasts increased in number with the initiation of enamel secretion. • The hydroxyapatite crystals are deposited more or less parallel to each other and interdigitate with the crystals of dentin in this initial layers which appears structureless (rodless). • As this first increment of enamel is formed, the ameloblasts begin to move away from the dentin surface (outward), and, as they do, each cell forms a conical projection called Tomes processes.
Secretory stage • When the tomes process is established, the enamel matrix is formed a rods, as the secretion of enamel protein becomes confined to two sites. • First site involves secretion from the proximal sites of Tomes process and forms interrod enamel. • Second site involves secretion from the distal sloping portion of Tomes process which later fills this pit with matrix. These pits are called enamel rods. • The difference between rod and interrod enamel is not chemical, but in the orientation of crystals. At planes where crystals of the rod meet those of interrod at sharp angels.
Maturative • This stage occurs after most of the thickness of the enamel matrix in the occlusal or incisal area has been formed; while in the cervical parts of the crown, the enamel matrix formation is still progressing. During this stage, the following changes occur: • The ameloblasts undergo significant reduction in the height and a decrease in its volume and organelle content. • Next the water and organic materials are selectively removed from the enamel while the additional inorganic material is introduced.
Smooth-ended Ruffle-ended Amelogenesis - Maturation Stage Ameloblasts incorporation of inorganic material exit of protein fragments & water Ameloblasts
Protective • After complete formation and mineralization of enamel, the ameloblasts form 3-4 layers of stratified epithelium that cover the enamel and called reduced enamel epithelium. • This reduced enamel epithelium protects the enamel by separating it from the connective tissue until the tooth erupts.
Desmolytic stage • Reduced enamel epithelium has the function of secreting desmolytic enzymes which cause degeneration of the connective tissue that separates the tooth from the oral epithelium.
Enamel Rods • The number of enamel rods ranges from 5 million in the lower lateral incisors to 12 million in the upper first molars. • The course of individual rod is wavy (except in cervical enamel, where the rods have straight course). • The length of most rods is greater than the thickness of enamel because of the oblique direction & the wavy course of the rods. • The rods located in the cusps, the thickest part of the enamel, are longer than those at the cervical areas of the teeth.
Enamel Rods • The diameter of the rods increases from the dentinoenamel junction toward the surface of the enamel at a ratio of about 1:2. • Have a clear crystalline appearance. • In cross sections of human enamel, many rods resemble fish scales. • The most common pattern of cross section is a key-hole. • The bodies of the rods are nearer occlusal & incisal surfaces, whereas the tails point cervically.
Rod sheath • It is the peripheral part of enamel rod forms an incomplete envelope around the prisms. It is less calcified than the rod itself.
Inter-rod substance • The enamel rods, which are not in direct contact with each other, are cemented together by inter-rod substance. • In human teeth, it appears to be minimum or absent in certain areas.
Incremental lines of RETZIUS • Appear as brownish bands in ground sections of the enamel. • Illustrate the successive apposition of layers of enamel during the formation of crown. • In longitudinal sections they surround the tip of the dentin. • In transverse sections of a tooth, they appear as concentric circles.
Neonatal Line • This is one of the brown striae of Retzius which is present only in the deciduous teeth and the first permanent molar. • This line separates the enamel which is formed before birth from that formed after birth. It is usually associated with the disturbance in the enamel formation produced at birth, due to the abrupt change in nutrition and environment.
Hunter- Schreger bands • The bands of Hunter and Schreger are an optical phenomenon produced by changes in direction between adjacent groups of rods. These bands are seen in longitudinal ground sections by oblique reflected light and are found in the inner two thirds of the enamel. They appear as alternating light and dark bands.
Gnarled Enamel • Over the cusps and incisal edges the rods appear twisted around each other in a complex arrangement known as gnarled enamel. Functionally, changes in rod directions between different layers may increase the strength of the enamel, making it less prone to fracture and more resistant to wear.
ENAMEL SPINDLES • Before formation of enamel, some developing odontoblastic processes extend into the ameloblasts layer and when enamel formation begins they become trapped to form enamel spindles.
ENAMEL TUFTS • Arise at the dentinoenamel junction & reach into the 1/3-1/5 the thickness of enamel. • Resemble tufts of grass when viewed in ground sections. • Consists of hypocalcified enamel rods & interprismatic substance.
Enamel Lamellae • Lamellae are thin hypomineralized sheets that extend from the enamel surface toward the DEJ junction and sometimes penetrate into the dentin. They are best seen in transverse sections of tooth. • May be a site of weakness in a tooth & may form a road of entry for bacteria that initiate caries.
Enamel Lamellae • Lamellae are of three types: • Type "A" : represent hypomineralized enamel rods, they occur developmentally and are filled with enamel protein. • Type "B" : represent cracks that are produced during development at planes of tension, and are filled with cellular debris, probably the remnants of the enamel organ. • Type "C" : are also cracks but they are produced after eruption, these are filled with organic debris from the oral cavity.
DENTINOENAMEL JUNCTION • The junction between enamel and dentin is seen as a scalloped border, with the convexities of the scallops are directed toward the dentin. • This arrangement, increase the surface area, and the adherence between the two tissues.
SURFACE STRUCTURES1-Perikymata • They are transverse, wavelike grooves, believed to be the external manifestations of the striae of retzius. • They are continuous around a tooth & usually lie parallel to each other & to the cementoenamel junction. • Their course is usually fairly regular, but in the cervical region it may be quite irregular.
2-ENAMEL CUTICLE • primary enamel cuticle covers the entire crown of the newly erupted tooth. • Is probably soon removed by mastication. • Is secreted by the ameloblasts when enamel formation is completed.
3- Rodless enamel • It is found at the enamel surface, has a thickness of 30µ and there may be also a very thin layer adjacent to the DEJ. It occurs because of the absence of Tome's processes on the ameloblasts responsible for the development of enamel rods. • It consist of closely packed crystals that are parallel to one another and perpendicular to the incremental lines of Retzius. This layer is more highly mineralized than the bulk of enamel beneath it.
4- Cracks • They are fissure like structures, found in all enamel surfaces. The extend for varying distances along the surface. They are actually the outer edges of enamel lamellae. By decalcification of enamel, cracks completely disappear.
Age changes in enamel A- permeability the enamel becomes gradually less permeable by age, the change being confined to the outer surface of old enamel the change is due to alteration in the organic part of enamel crystals may acquire more ions and increase in size by age reducing the size of pores between them this lead to decrease permeability.
age changes in enamel B-color changes of the tooth Teeth darken with age due to addition of organic material from the environment, in addition to the tobacco stains and that of tea and coffee, also attrition lead to tinning of the enamel surface reflecting the yellow color of underlying dentin
Age changes in enamel C-attrition • the most frequent age change of enamel is attrition of occlusal and proximal contact areas as a result of mastication it varies according to : • nature of diet • hardness of teeth • certain oral habits • nature of occlusion
The outer manifestation of straie of retsiuz is the perikymata which become obvious when enamel worn
Clinical considerations of enamel • Enamel can not repair itself. • Dental caries. • Fluoridation. • Effects of dental procedures 1- Dental restorations 2-Acid-etching technique
Clinical consideration • Enamel can not repair itself, because the ameloblasts are lost after the enamel has been laid down, but remineralization can occur in the surface enamel. • Diseased, fractured, or otherwise damaged enamel can only be repaired through operative procedures.
Dental caries Although enamel is the hardest tissue in the human body, it is permeable to some fluids, bacteria, and bacterial products of the oral cavity. Enamel exhibits cracks, and microscopic spaces within and between rods and crystals, allowing penetration.
Enamel can lose mineral substances due to unfavorable long term conditions involving low pH and the presence of carbohydrates and microorganisms which cause caries changes. Fluoridation
To prevent demineralization of dental hard tissues, the enamel structure needs to be remineralized by supplementing fluoride, phosphorus, calcium, and other ions into the enamel apatites. It can be performed by application of toothpastes supplemented with cariostatic ions and/or placing fissure sealants or varnishes on the total enamel surface.
Effects of dental procedures… 1- Dental restorations • Most dental restorations involve the removal of enamel. • The purpose of removal is to gain access to the underlying decay in the dentin or inflammation in the pulp.