Download
1 / 54

E N D
PLEURAL PLEURAL EFFUSION EFFUSION Professor mohammed Ahmed Bamashmos
Outline • Definition • Anatomy and mechanisms • Etiology and physiology • Manifestation • Imigeologic findings • Laboratory findings • Diagnostic procedures • Corresponding diseases • Treatment
? • Howdoes pleural effusion generate • Howto diagnose pleural effusion • What are corresponding diseases
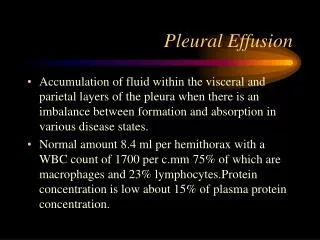
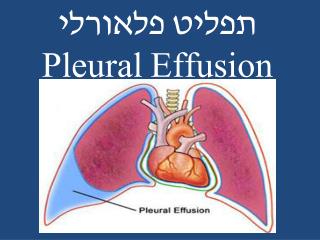
Definition Pleural effusion is a condition that has an accumulation of an excessive amount of fluid in the pleural space that has very little fluid for lubrication in it normally.
Anatomy & Mechanisms consist of a layer of mesothelial cells connective tissue vessels lymphatics classified as prietal & visceral
• • Parietal pleura covers the surface of chest wall diaphragm mediastinum receives blood from systemic circulation contains sensory nerves • Visceral pleura covers and adheres tosurface of both lungs receives blood from pulmonary circulation contains no sensory nerves
Parietal & Visceral pleurae Visceral pleura Parietal pleura
• two pleural surfaces are separated by a potential space —a pleural space --exists 5-10ml of fluid • mean pressure in space is – 0.5 cmH2O
parietal (systemic) space visceral (pulmonary) hydr 30 11 5 neg.press. 8 coll. coll 34 34 in out = = 30+5+8-34=9 34-11-5-8=10 Pleural Effusion Circulation
Etiology & Physiology MajorForces • Hydrostatic forces↑ • Colloid oncotic pressure ↓ • Permeability ↑ • lymphatic flow ↓ • Movement of peritoneal fluid
1. Hydrostatic pressures↑ • Congestive left heart failure • Right ventricular failure • Constrictive pericarditis • Obstructed upper cava Pulmonary circulation Systemic circulation Causes → hydrostatic forces↑→ filtrates → protein-poor transudates
2. Colloid oncotic pressure ↓ • Hypoalbuminemia • Cirrhosis • Renal disease syndrome • Acute glomerulonephritis • Mucosal edema Causes → oncotic pressures↓→ filtrates → protein-poor transudates
3. Permeability ↑ • Inflammation (TB, pneumonia) • Rhumatic diseases (SLE, rheumatoid) • Malignancy (metastasis, mesotheliomas) • Embolism Causes → pleural capillaries are damaged → infiltration↑→ reasorption are broken down → protein-rich exudates
4. Disorders of lymphatic flow in parietal pleura • malignancy • abnormal lymphatics development Malignant lymphatics obstruction → lymphatics absorption ↓ → protein-rich exudates Abnormal development → protein-poor exudates
5. Movement of peritoneal fluid Transudates or exudates into the pleural space appear to transverse the diaphragm either through lymphatics or through small holes in the diaphragm 6. Trauma Aortic tumor → bloody Esophagus → purulent Thoracic duct → a milky
parietal (systemic) hydr space visceral (pulmonary) coll Permeability Lymph Peritoneal leakage effusion Physiology of Pleural Effusion
Manifestation • Pleural pain unilateral sharp accentuated • Dyspnea • Respirations rapid shallow • Dullness or flatness • A pleural friction rub • Decreased or absent breath sounds
Imagiologic Findings 1. Radiological findings • a Blunting costophrenic angle (less) • a concave shadow with its highest margin along the pleural surface (medium, large) • a pseudotumor (loculated) • a “high diaphragm” with a peak more lateral than usual (subpulmonic) • An air-fluid level (hydropneumothorax)
air-fluid level Hydropneumothorax
2. Ultrasonic examination • Detect liquid • Probe something covered by liquid • Provide location for thoracentisis 3. CT • Identify different liquids • Recognize masses in mediastinum paratrachea lung pleura
Laboratory Findings 1. Appearance:by thoracentesis transudates--clear proportion <1.016~1.018 exudates ---- unclear proportion >1.018 purulent ----- unclear white, black, bloody putrid odor, ammonia odor
2. Cells • Total transudative <100?106/L (Lymphocytes and mesothelial cells) • WBC transudative -- <100 ? exudative – >500 ? purulent -- >10,000 ? acute inflammation— N TB, malignant—L parasites, reumatic — EOS
• RBC tumor, TB -- > 5 ?109/L trauma, tumor, embolism ------100 ? • Carcinomatous cells • Chromosome • Lupus 3. Proteins • transudate---- <30 g/L Rivalta test (+) • exudate ------- >30
4. Glucose • transudate --- > 3.34mmol/L • exudate ------ < 3.34 • purulent ------ < 1.11 • reumatic ----- < 0.12 5. Pathologic examination by biopsy • TB nodule • Tumor cells ?
Diagnostic Procedures 1. Determine effusions • History and manifestation pleural pain – unilateral, sharp, worsening dyspnea ------ chest tightness (0.3~0.5 L) dyspnea (large) physical exam -- rubs flatness/dullness absent/decreased BS
• Imageologic findings Radiological examination small,medium, large loculated subpulmonic air-fluid level CT Ultrasonic examination
2. Recognize causes • History and PE TB – younger, fever malignant – elder, bad condition, lymphanodes inflammatory – chest pain, fever heart failure – right heart failure reactive – enlargement of liver
• Pleural fluid analysis Thoracentesis Lab Transudates / Exudates apperance cells proteins glucose
Thoracentesis • Goals: diagnosis therapy • Indications: pleural effusion • Diagnostic: 50-100ml Therapeutic: < 600ml at 1st <1000ml at one time) • Contraindications: bleeding diathesis a small volume mechanical ventilation • Complications: pain bleeding pneumothorax infection spleen/liver puncture
Correlation of pleural fluid findings and causative diseases Fluids Diseases Transudative heart failure, renal syndrome, cirrhosis Exudative TB, malignancy, infarction, rheumatic Purulent secondary infection Bloody trauma, malignancy, infarction, TB, pneumothorax White chyle, cholesterol, lymphoma Black aspergillosis Yellow green rheumatoid pleurisy
• Pleural biopsy most frequently in TB and malignancy a specific pathologic diagnosis localize with ultrasound for sufficient pleural fluid • Thoracoscopy • An open pleural biopsy
Corresponding Diseases 1. Effusion due to heart failure • History of heart disease • Palpitation, dyspnea, arrhythmia • Enlarged heart , liver, edema • Bilateral effusion usually larger on the right side • Transudates
2. Hepatic hydrathorax • Cirrhosis and acites • Liver function • Hypoalbuminemia • Ultrasound • Transudates
3. Tuberculous pleuritis • Most common cause of an exudative • Fever, weight loss, dyspnea, and/or chest pain • Positive result of PPD skin test • Exudative • Pleural biopsy
4. Effusion secondary to malignancy • Second most common cause • Three frequently seen tumors lung carcinoma breast cancer a lymphoma • Diagnosis is made by thoracentesis biopsy thoracoscopy
5. Mesothelioma • including benign or malignant • Persistent chest pain • Bloody effusion • Different film representation benign ------ smooth loculated malignant -- generalized and irregular • Therapy benign ------ surgical treatment malignant -- no effective treatment
6. Effusion with pneumonia • The extent varies widely • Pleural involvement by nonbacterial, nontuberculous infections is uncommon • Empyema fluid should be completely removed
Treatment 1. Effusion due to heart failure • Treat underlying diseases • Diuretics • Vasodilators • Extract liquid
2. Hepatic hydrathorax • Treat underlying diseases • Correct liver function • Enhance serum albumin • Take out liquid for alleviation
3. Tuberculous pleuritis • Chemotherapy • Take out liquids <1L / time 2~3 times / week thoracic reaction --- cease, adrenaline pulmonary edema – O2, corticoids, diuretic • Corticosteroid severe large amount 4-6 weeks
4. Malignant effusion • Anti-tumor chemotherapy systemic local • Drainage thoracentesis closed • Support
5. Empyema • Antibiotics systemic local • Drainage thoracentesis closed • Surgery • Support