Download
1 / 49
490 likes | 756 Views
Helping Kids to Health The role of Iowa public schools Collaborators Iowa Dietetic Association Iowa Dental Hygienists Association Iowa School Food Service Association Iowa Fit Kids Coalition ISU Extension Discussion Objectives To understand and describe

E N D
Helping Kids to Health The role of Iowa public schools
Collaborators • Iowa Dietetic Association • Iowa Dental Hygienists Association • Iowa School Food Service Association • Iowa Fit Kids Coalition • ISU Extension
Discussion Objectives To understand and describe • Three examples of health problems that can be prevented • How the school environment impacts health and nutrition • Policy changes that can impact health of students
Invest in a Child’s Health To help his/her… • Ability to learn • Physical ability • Appearance • Social opportunities • Success in school and future employment Health is key to a long and productive life!
Preventable & Interrelated Health Problems • Obesity • Dental Caries • Osteoporosis • Psychosocial Concerns
Overweight and Obesity • Obesity has been related to changes in our lifestyle, including diet and physical activity • Efforts to lose weight have proven unsuccessful for many adults. • Obese children are 43.5 times more likely to have at least 3 cardiovascular risk factors. Nicklas, 2001 • As many as 45% of children newly diagnosed with diabetes have type 2 diabetes.
The Problem of Childhood Overweight • Complex …but simple • Cannot ignore that one cause is caloric intake that exceeds caloric expenditure. • Experts recommend that we concentrate on preventing overweight.
No Simple Answer to the Obesity Epidemic Glycemic Index Food Industry TV Sugar Candy Decreased PE in Schools Genes Energy Density ObesityEpidemic Soft Drinks Decreasing Physical Activity Pouring Contracts Junk Food School Feeding Restaurants Poor Parenting Fast Food Working Mothers Computers Poverty Nicklas, TA, 2003
Genetic vs. Environmental Obesity gene • Children have higher risk of obesity when either one or both parents are obese. • Obesity associated with genetic syndromes What has changed? … • “Gene pool” has not changed • Environment: has changed
Dental Health • Tooth decay is the most common chronic disease among children--5 times more common than asthma. • An estimated 51 million school hours per year are lost due to dental related illness • Children with chronic dental pain are unable to attend to school work. (Oral Health in America: A Report of the Surgeon General, 2000) • Poor oral health tied to decreased school performance, poor social relationships and less success later in life
Dental Health • 20% of low income children in Iowa have untreated decay in permanent teeth. • 68% of low income children have a history of decay compared to 52% of higher income children. • 56% of children participating in the IDPH dental sealant programs have a history of decay.
What Dentists are Seeing “Pre-fluoride” conditions of mouths
Bone Health • Bones are formed during childhood and adolescence. • Milk and dairy products are the best sources of calcium needed to form bones. • Lack of calcium in adolescence could lead to bone health in later years. • Weight bearing exercise is an important factor in bone formation and retention.
Bone Health • Osteoporosis is “a pediatric disease with a geriatric outcome” • Physically active girls who consume soft drinks have more bone fractures Wyshak, G, Arch Pediatr. Adolesc. Med, 2000; 154:610-613. • Over 10 million men & women are estimated to have osteoporosis in 2002; another 33.6 million have low bone mass and are at risk for osteoporosis. National Osteoporosis Foundation http://www.nof.org/osteoporosis/state.htm
Psychosocial Concerns of Poor Health • Lowered self esteem • Body image disturbances • Depression • Poor academic performance • Increased behavior problems
Why be Concerned? • 70 to 80% of overweight teens become overweight as adults. • Poor diet/inactivity in adults causes 300,000+ deaths annually. • Osteoporosis decreases mobility and increases pain and has been reported in women.
What has Changed? Physical Activity • 22% children did not participate in moderate or vigorous physical activity • 20% were not enrolled in physical education class • 86% did not attend physical education class daily (Youth Risk Behavior Survey, CDC, 2000)
Physical Activity • Physically fit children perform better academically – California schools • NASPE recommends 150 minutes/week of physical education • Qualified teachers can ensure safety and teach appropriate activities that are enjoyable, develop motor skills and maintain health related fitness.
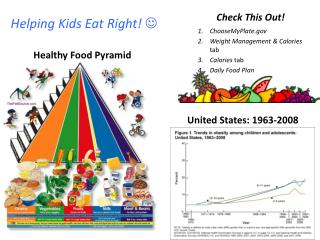
What has Changed? Children’s Eating Habits • Only 2% of kids meet all Food Guide Pyramid Recommendations • 16% do not meet any recommendations • 12% report skipping breakfast • Only 11% eat a breakfast that contains three food groups and provides >25% of RDA for energy
Compared to Recommendations • 84% of kids eat too much fat; • 91% eat too much saturated fat • Only 15% get enough fruits • Only 20% get enough vegetables • Only 30% get enough milk • Only 19% of girls aged 9 to 19 years of age meet calcium recommendations
Soft Drinks: The Facts Who drinks soft drinks? • 50% of all Americans • 65% of adolescent girls • 74% of adolescent boys Borrud, et al., Community Nutrition Inst, 1997
Plaque pH 7.0 6.0 5.0 4.0 critical pH 0 20 40 60 80 100 120 minutes Acidity in the mouth after drinking a sweetened beverage single glucose rinse
Plaque pH 7.0 6.0 5.0 4.0 critical pH 0 20 40 60 80 100 120 minutes Acidity after repeated exposures to a sweetened beverage First sip Second sip Third sip Fourth sip
Double Trouble: pH and Sugar Content Acidity (pH) Sugar (tsp) Water 7.00 0.0 Diet Coke 3.39 0.0 Mountain Dew 3.22 11.0 Diet Pepsi 3.05 0.0 Gatorade 2.95 3.3 Coke 2.53 9.3 Pepsi 2.49 9.8
Challenges for Change • Public Health cannot compete with industry’s advertising budget • Mandated changes are controversial • Lifestyle changes are difficult for individuals Aim for small improvements over time
Hope for Change • Simple policies can promote health • Activity promotion fits in well with fun school events • Alternative fund raisers • Children adapt to new ideas and experiences • School provides a venue for experiencing new tastes and activities
Why Change the School Health Environment? Education is a process of planning and preparing for a successful future
Why Schools? • Schools play a role in demonstrating to the parents and community the elements that lead to a successful and healthy lifestyle • Children spend time in school
Roles for Schools • Continue to provide nutritionally balanced meals to children • Coordinate nutrition education with opportunities to eat healthy foods. • Support nutrition education messages in the overall school environment. • Provide tools for lifelong physical activity and healthy eating.
Challenges Nutrition for Schools in the 21st Century • Budget constraints for schools and school meal programs • Shortened meal times • Weak regulations for physical activity and health in schools • School meals must compete with offerings both on and off campus • Foods sold in competition with the school lunch program for revenue are often of minimal nutritional value
Carbonated Soft Drink Sales Challenge: • Source of revenue for schools • Competes with goals & revenue of school lunch • Conflicts with nutrition education message • USDA regulations only limit placement & timing of vending machines
Carbonated Soft Drinks in the School Challenge: • Potential to disrupt the classroom • Sugar intake gives children a surge of energy followed by a drop of energy. • More than 51 million school hours are lost each year to dental-related illness.
American Dental Association Policy: 2000 House of Delegates : • oppose contracts that offer increased access of soft drinks to children and influence their consumption patterns. • calls for continued monitoring of scientific facts and data on the oral health effects of soft drinks. (2000)
Taking a Position on Healthy School Environments • American Dietetic Association • American Academy of Pediatrics • Society for Nutrition Education • Centers for Disease Control and Prevention • Center for Food and Justice • American School Food Service Association
Meeting the Challenge: • Create school meal advisory teams of students, parents and teachers to assist in selected menu items. • Survey students on preferred foods. • Educate students about serving sizes • Employ economies of scale to increase revenue • Ensure that food sale revenues for competitive foods are credited to the school food service
Meeting the Challenge: • Develop positive, healthy options for vending, school stores, cafeteria environment • Ask soft drink companies to market healthier alternatives. • Provide water, 100% juices, milk and soy drinks
Meeting the Challenge: • Require closed campuses during lunch periods. • Competitively price healthy foods • Sell items that increase physical activity: pedometers, water bottles. • Establish relationships with local food producers • Participate in school gardening projects
Meeting the Challenge: • Ensure that adequate time and space is available for all children to eat comfortably • Schedule recess before lunch • Encourage teachers and staff to eat with children
Meeting the Challenge: • Limit use of food and candy as a reward. • Encourage fund raising efforts associated with healthy lifestyles • Provide daily recess • Plan physical education that is inclusive of all students, including those with disabilities
Meeting the Challenge: • Fruit & Vegetable Pilot Project • 25 schools in Iowa • Free fruits & vegetables provided throughout the day • Children learned new foods; enjoyed them • Decreased use of vending machines • Positive influence on school environment
Resources School Health Index • http://www.cdc.gov/nccdphp/dash • http://www.cdc.gov/nddphp/dnpa Changing the Scene • www.fns.usda.gov/tn Fit Healthy & Ready to Learn • http://www.nasbe.org/HealthySchools/healthy_eating.html
More Resources Team Nutrition • www.fns.usda.gov/tn Healthy Schools Summit • www.actionforhealthykids.org Alternative ways to raise money • http://www.scn.org/edu/cccs/ • www.commercialfree.org
Conclusions • Schools can positively impact the health of students • A number of options are available to implement school health programs. • A number of tools are available to evaluate environments within schools
Acknowledgements Thanks to the following persons who have provided expertise and visual support for this presentation Dr. Michael Kanellis, DDS, MS Dr. Jonathan Shenkin, DDS, MPH Linda Snetselaar, RD, PhD Eva Tsalikian, MD University of Iowa School of Dentistry, College of Public Health and College of Medicine
Evaluation • Facilitators • Provide RD’s not yet enrolled on Professional Developmental Portfolio, CDR reporting form: http://www.cdrnet.org/pdfs/RC-4.pdf • Please complete evaluation form (note page) & return • Send any additional comments