Download
1 / 18
190 likes | 405 Views
The role of the Childhood TB Subgroup in vaccine research. Gunnar Bjune TB in the 21st Century Consortium. Not to loose what we have (BCG). Reduces child mortality Prime the immune response for strong Th1 reactivity Protects against allergy Modulates the immune response

E N D
The role of the Childhood TB Subgroup in vaccine research Gunnar Bjune TB in the 21st Century Consortium
Not to loose what we have (BCG) Reduces child mortality Prime the immune response for strong Th1 reactivity Protects against allergy Modulates the immune response to ags towards Th1 pattern, not Th2 The gateway to EPI Quality of MC services Administered at birth (institutional delivery, registration, vaccination card)
BCG coverage • Institutional delivery Quality, referral services/transport • Side effects and other SEFIs Control, management, registration/reporting • Evaluation
BCG and immune deficiencies • HIV Mothers’ HIV status • Measles Lack of maternal antibodies • Malnutrition/immaturity Low birth weigth babies
Watch introduction of ”emerging successful Mtb strains” • Relative strain prevalence in <15 yrs versus >40 yrs TB pats TB diagnosis in children, gastric lavage • Efficacy of BCG vaccination Case-control studies with strain typing TB meningitis and BCG status
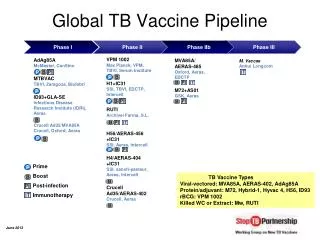
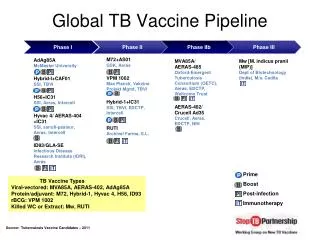
New anti-TB vaccines • ”BCG boosting vaccines” • Mtb specific antigens + new adjuvance • Live vectors with rec. Mtb antigens • Vaccines to prevent reactivation of latent TB (therapeutic/post-exposure) • ”2nd generation” anti-TB vaccines (resistance/escape)
Diverse TB epidemiology and diverse vaccine needs • A: Stable, mainly reactivation of latent TB, low HIV prevalence (small overlap) • B: Increase, recent infections, low HIV (more overlap) • C: Increase, recent infections, high HIV (full overlap)
Overlap.. (age/socioec./gender…) TB • Norway • Russia • Tanzania HIV
A: Stable, mainly reactivation of latent TB, low HIV prevalence (small overlap) • High cost-effectiveness of coordinated preventive programs • Childhood cases few and mainly among household contacts • Full coverage of newborns with BCG • Post-exposure vaccine preferably as a BCG boostering strategy (previous BCG coverage?)
Overlap.. (stage of the epidemics) % sp+ TB Costs HS Cost Cost/ effective Transmission Early Late
The cost of human immunodeficiency virus co-infection to health services in Sudan. Asma Elsony et al. 2004 • 4% of TB pts HIV+ • Total cost of management of HIV+ pts was 6% of all costs for TB management. • Marginal cost attributable to HIV-positivity was 0.9% of the total cost. • Still total cost significantly higher for HIV+/ HIV- TB ptss ($ 105.1 vs $ 73.9, p=0.003).
Cost… continued • No sign. difference in costs between HIV+ / HIV- TB pats for: diagnostic tests, drugs and management of adverse reactions • Slightly more side effects of treatment among HIV+ / HIV – TB pats (14% vs 9.6%). • Cost difference due to more hospitalization (mortality and morbidity) of HIV+ / HIV- TB pts ($190.8 vs $141)
B: Increase, recent infections, low HIV (more overlap) • High cost-effectiveness of coordinated preventive programs • More childhood cases, but HIV neg. (TBmeningitis in < 5yrs old) • Full coverage of newborn BCG • ”2nd generation” anti-TB vaccines (prevalence of emerging successful strains?)
C: Increase, recent infections, high HIV (full overlap) • Cost-effectiveness of coordinated preventive programs low • Childhood cases many, community contacts (more HIV pos.) • BCG to newborns with caution • ”2nd generation” anti-TB vaccines, no live vector
TB meningitis (BCG failure?) • Efficiently prevented by BCG • No effect of environmental mycobacteria < 1 y of age • Diagnostic performance, recording, reporting? • Strain epidemiology?
Emerging successful strains • Rate in TB pats < 15yrs / <40 yrs • RFLP + spoligotyping + ? • Culture (gastric lavage)? • BCG coverage registration / reporting • Other selective factors? (drugs, BCG, HIV, urbanization, MOT..)
What to do??? • Meet EPI • Support full coverage of BCG to newborns (quality of services, evaluation, documentation) • Meet NTP • TB meningitis, strains from pts < 15 yrs (quality of services, evaluation, documentation) • BCG status of TB pts (by scar) recording • Meet NHAP • HIV+ among TB pts; TB among HIV+s (overlap) • Meet the vaccine carpenters and funders and tell them what you need (post-exposure and second generation ignored)