Download
1 / 32
320 likes | 804 Views
. Background. Background. Lowering LDL-cholesterol has become one of the integral components of standard of care in coronary artery disease patients.ATP III recommends the target LDL-C of 70mg/dl in patients with known h/o CAD.Scandinavian Simvastatin survival study (4S) in 1994 with Simvastatin 20 to 40mg/day in CAD patients showed 30% reduction in total mortality.In the context of above, 4 large outcome trials have tested the effect of varying degrees of LDL cholesterol which incl9458

E N D
1. Journal Club
2.
Background
3. Background Lowering LDL-cholesterol has become one of the integral components of standard of care in coronary artery disease patients.
ATP III recommends the target LDL-C of
70mg/dl in patients with known h/o CAD.
Scandinavian Simvastatin survival study (4S) in 1994 with Simvastatin 20 to 40mg/day in CAD patients showed 30% reduction in total mortality.
In the context of above, 4 large outcome trials have tested the effect of varying degrees of LDL cholesterol which include PROVE IT- TIMI22, A to Z trial, TNT trial and IDEAL trial.
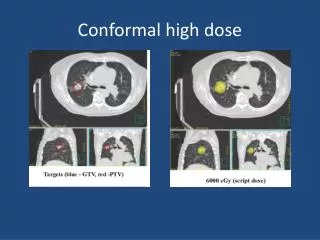
4. Background .. IDEAL trial was set to examine the effect of intensive lipid lowering on cardiovascular mortality and morbidity with high doses of statins vs. conventional method of low to moderate doses.
Hypothesis:
Intensive lowering of LDL cholesterol with atorvastatin at the highest recommended dose would yield incremental benefit compared with the moderate, most widely used dose of simvastatin.
5.
OBJECTIVE
6. To compare the effects of 2 strategies of lipid lowering on the risk of cardiovascular disease among patients with myocardial infarction
7.
Study Design
8. Study Design Multicenter, prospective, randomized, open-label, blinded end-point classification trial.
Conducted at 190 ambulatory cardiology centers in Denmark, Finland, Iceland, Netherlands, Norway and Sweden.
Recruitment and randomization- March 1999 to March 2001
Follow up until March 2005.
Total no. screened- 9689
9. Initial Screening Records of the patients were screened for eligilibility criteria
Eligible patients invited for screening;
Written informed consent
Study approved by national review boards of respective countries.
Eligibility criteria:
Men and women less than or equal to 80 yrs with a definite history of myocardial infarction and who qualified for statin therapy (LDL >70).
Patients previously treated with statins qualified if they had not already had a titration to a dose higher than the equivalent of simvastatin 20mg/day.
10. Exclusion criteria Any known contraindications to statin therapy
Previous intolerance to statins in low or high doses
Liver enzyme > 2 times the upper limit of normal
Pregnancy or breastfeeding,
Nephrotic syndrome,
Uncontrolled diabetes mellitus,
Uncontrolled hypothyroidism,
Plasma triglyceride levels higher than 600 mg/dL
Congestive heart failure (NYHA class IIIb or IV),
Hemodynamically important Valvular heart disease
Gastrointestinal conditions affecting absorption of drugs
Treatment with other drugs that seriously affect the pharmacokinetics of statins,
Treatment with other lipid-lowering drugs
11. Study Design Randomized to receive Atorvastatin 80mg/day or simvastatin 20mg/day.
Subjects allocated to either arms in the blocks of 24 via central interactive voice response system.
Follow up:
12 weeks, 24 weeks and every 6 monthly.
Fasting lipid and lipoprotein levels measured at each visit.
Dose adjustments made at 24 weeks (simvastatin to 40mg/d if LDL > 190 and atorvastatin to 40mg/day for adverse events).
Liver enzymes at baseline, 12, 24 weeks and yearly thereafter.
Results not revealed to study personnel unless dose adjustments are required.
12. Study Outcomes
13. Study outcomes Primary outcomes:
Time to first occurrence of a major coronary event�
Coronary death.
Hospitalization for nonfatal acute myocardial infarction.
Cardiac arrest with resuscitation.
14. Study outcomes (contd..) Secondary outcomes:
Major cardiovascular events defined as any primary event plus stroke.
Any CHD event defined as any primary event, any coronary revascularization procedure, or hospitalization for unstable angina
Any cardiovascular events defined as any of the (1) or (2) plus hospitalization with a primary diagnosis of congestive heart failure and peripheral arterial disease, defined as new clinical diagnosis or hospitalization for such disease.
In addition, individual components of the composite end points were also prespecified as secondary outcomes, as was all-cause mortality.
15. Statistical Analysis
16. Statistical Analysis
The trial was anticipated to show a 21% relative risk reduction in the primary outcome variable with 90% power over 5 years.
Kaplan-Meier hazard rates were used to examine incidence over time and the log-rank test was used to assess group differences.
The final statistical analysis was performed by sponsor.
All analysis based on intention to treat principle.
A data and safety monitoring board performed interim analysis when approximately 50% and 75% the predetermined final number of 774 patients had experienced primary end point.
17.
Results
21. Results Median follow up time was 4.8 yrs.
Dosage adjustments were made to 900 patients in Simvastatin arm and 250 patients in atorvastatin arm. This increased to 1034 and 587 respectively by the end of the study.
Overall adherence- 89% in atorvastatin and 95% in simvastatin group.
Mean reduction in LDL in simvastatin was 33% by 12 weeks while it was 49% in atorvastatin arm; Compare it to 104 in the simvastatin and 81 in the atorvastatin arm by the end of treatment period.
TGs and Cholesterol levels decreased while HDL slightly higher in simvastatin group.
22. Results� In Dec 2004, 702 patients had attained primary end point. It was, thus, calculated that the protocol specified target of 774 patients would be finished by Apr 2005. 874 patients had actually experienced a primary end point by that time. (end point classification trial).
24. Results.. HR of atorvastatin vs simvastatin was 0.89 in primary end point indicating a relative risk reduction of 11% with rapid lipid lowering therapy.
Significant risk reduction was observed to be with non fatal MI and composite end point of major cardiovascular event including stroke.
All cause mortality did not show any significant difference between the two arms.
No significant differences in the frequency of serious clinical adverse experiences. Elevation of liver enzymes occurred more frequently in atorvastatin group though there is no evidence of clinical liver disease.
Similarly though myalgias occurred more in atorvastatin arm, myopathy rates were very low in both the arms.
25. Results..
26.
Conclusion
27. Conclusion In conclusion, Atorvastatin 80mg decreased LDL by 33% when compared to simvastatin arm with 16% change.
In spite of the above, there is no significant benefit shown by rapid lowering of LDL-C in persons with prior MI in terms of mortality, including cardiovascular and non cardiovascular.
However, significant reductions in non fatal MI and secondary outcomes were noted.
Numerically speaking, aggressive lowering of lipid in patients with previous MI may prevent 68 first cardiovascular events per 1000 persons over 5 years.
Some explanations for the failure to show significant reduction include low adherence in atorvastatin arm; premature attainment of primary end points (4.8 yrs vs anticipated 5.5 yrs); possible effect of simvastatin on HDL.
28. Weakness..
Not a double blinded but a open end classification trial
Open label design, though close to real life design, can raise the possibility of physician bias esp. in case of hospitalization for unstable angina etc
More observed adherence to simvastatin (as many had pre randomization simvastatin).
Complicated secondary outcomes.
29.
Other Outcome Trials
31. Letter to the editor Statins, Diet, and Low Cholesterol To the Editor: In his Editorial discussing recent trials of statins, Dr Cannon did not address some of the remaining questions. First, the 4 contemporaneous trials discussed (PROVE IT-TIMI 22, A to Z,TNT, and now, the IDEAL trial) have failed to show a reduction in all-cause mortality despite the use of aggressive and higher doses. Second, while previous concerns about increased incidence of cancer and other noncardiac deaths have been somewhat allayed in careful post hoc analysis in these studies, the number of participants who developed cancer in each of these trials may have been too small to find significant differences.
In addition, with the A to Z and IDEAL trials showing no difference in primary outcomes, attributes that may vary among statins, such as pleiotropic or anti-inflammatory effects, may be more pertinent in patients with acute coronary syndrome. Finally, there is a lack of prospective data in elderly persons, women, and patients with renal failure who have hyperlipidemia. These deficiencies in information about statins need to be acknowledged.
Rohit Arora, MD Saravanan Balamuthusamy, MD, MPH Department of Medicine Chicago Medical School at Rosalind Franklin University North Chicago, Ill
32. Thank you